Download
1 / 45
641 likes | 1.08k Vues
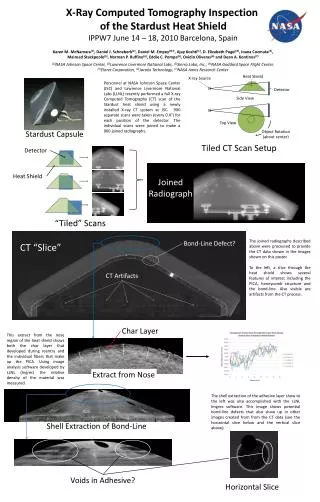
PET-CT in Lung Cancer: Positron emission tomography – computed tomography to whom, when ? Jann Mortensen, MD, DMSci Department of Clinical Physiology, Nuclear Medicine & PET, Rigshospitalet University Hospital of Copenhagen, Denmark Jann.Mortensen@rh.regionh.dk. Antalya, 26 april 2008.

E N D
PET-CT in Lung Cancer: Positron emission tomography – computed tomography to whom, when ? Jann Mortensen, MD, DMSci Department of Clinical Physiology, Nuclear Medicine & PET, Rigshospitalet University Hospital of Copenhagen, Denmark Jann.Mortensen@rh.regionh.dk Antalya, 26 april 2008
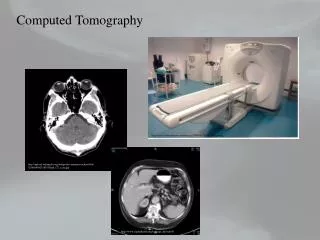
PET - CT CT PET Fused PET + CT Investigates functional changes in the body tissues and anatomy simultaneusly Anato-metabolic imaging
Physiology of FDG tumor uptake FDG signal in tumor is dependent on 1) delivery (blood flow), 2) transport into the cells (glut), and 3) phosporylation (hexokinase) FDG tumor uptake ~ number of viable cancer cells R.Wahl. Priciples and practice of positron emission tomography, 2002
Physiological uptake of FDG Brain Salivary glands Larynx Thyroid Heart GI tract incl liver Genito-urinary tract Bone marrow Lymphoid tissue Brown fat
Main indications for PET in lung cancer • Characterising pulmonary nodules which are borderline for malignancy on CT • And cannot be easily biopsied • Staging in NSCLC • Preoperative evaluation • N and M (nodes and metastasis) 55 studies with > 2000 patients with histologic or long-term follow-up Fischer BM, Mortensen J, et al. Lancet Oncol 2001;2:659-66
FDG-PET in solitary pulmonary nodules • Indeterminate single pulmonary nodule/mass on CT • Malignant or benign ? • N=16 studies • Sensitivity 0.96 (0,90-1,00) • Specificity 0.78 (0,69-0.95) • Size: 1-4 cm • 1474 nodules (JAMA 2001; 285: 914-24) • Only few nodules <1 cm:
FDG PET in >1 cm nodules • FDG-PET can discriminate between malignant / benign ≥ 10 mm solid pulmonary nodules !!! • FDG-PET has a high negative predictive value, can correctly exclude malignancy in the vast majority of nodules seen in daily practice. • ~ changes management in > 26 % of patients • A surgical procedure can be avoided, and a repeat CT • after 3 (6, 12 and 24) months can be used to confirm • the absence of growth. Lancet Oncol 2001; 2: 659-66 Lung Cancer 2004; 45: 29-30.
57 yr male with COPD 9 mm nodule found on high-resolution CT 18F-FDG PET
57 yr male with COPD transaxial coronal saggital Diagnosis and staging (PET suggests T1 N0 M0) attenuation corrected RH - PET / jm (ap) Fischer BM, Mortensen J, et. al. Nucl Med Commun 2004; 25: 3-9.
PET in ”The Danish randomisedlow-dose CT screening study of lung cancer” • Ongoing screening study in Copenhagen: • Included 4000 • Yearly CT vs. Control in 5 yrs • now 3 year • Value of PET in characterisingindeterminate SPN 6-15 mm detectedwithlow-dose CT • - all SPNsfollowed-upwithre-CT at 3 months to assessgrowth
PET in Danish randomised low dose CT screening PET positive case Initial 9x12x9 mm solid nodule in R3, PET positive + 2 N2 PETpos + CT growth -> Biopsi/Mediastinoscopy: T1N2M0(->Chemotherapy)
PET in Danish randomised low dose CT screening CT + PET axial a PET negative case 10 mm solid nodule in L3 PET negative CT stationary
PET data from CT- screening in Milano PET in 68 SPN >7 mm ~ 1,4% of 1.035 participants Danish study: Accurracy. 89% With PET : complete diagnostic workup <4 months at baseline and < 2 months at 2-5 yrs Jann Mortensen, klinisk fysiologi, nuklearmedicin og PET, Rigshospitalet
FDG PET in small nodules (<10 mm) • PET is promising as a tool in lung cancer screening with low-dose CT • [Lung Cancer 2004; 45:19—27] [Nucl Med Commun 2004; 25: 3-9] • [Am J Respir Crit Care Med 2005; 171:1378-83][Lancet 2003;362:593-79] • The interpretation of FDG-PET findings in subcentimetric nodules is at present unsolved • [Vansteenkiste JF. Lung Cancer 2004; 45: 29-30].
Staging T N M status (in one exam) • Conventional staging is inaccurate [Lancet 1996;347:649–653]. • PET for staging: • Staging the Mediastinum • PET more accurate than CT for detection of locoregional metastases • PET sensitivity >84%, specificity >89% • (18 prospective studies) • Detecting distant metastases: • PET sensitivity >90%, specificity >90% • and better than CT (17 prospective studies) • Change in management • >25% of patients (15 prospective studies) Preoperative staging with FDG-PET Oturai, Mortensen, Eigtved et al. J Nucl Med 2004;45:1351-7
Prospective study of Preoperative staging with PET vs. standard staging (CT, ultrasound, bone scanning/ biopsy) • 102 patients with resectable NSCLC, 6 months follow-up, • histopathological reference. • (N) metastasisSensitivitySpecificity • PET 91 % 86 % • CT 75 % 66 % (M) metastasis: PET identified distant metastases not found by standard methods in 11 of 102 patients: PET identified a different stage in 62 patients: stage was lowered in 20 and raised in 42 Pieterman et al. N Engl J Med 2000;343:254-61
Randomised study of PET staging • Effect parameter: no. unneccesary thoracotomy´s • 188 ptt. usual work-up +/- PET, 1 yr follow-up • 9 Deutch hospitals (1 dedicated PET center) • PET reduced the no. unneccesary thoracotomy´s: • PET 32 (41%) , + PET 18 ptt (21%) • For each 5 PET scans one unneccesary thoracotomy was avoided • reduced cost per patient with PET: > 1.000 EURO (PLUS study. Lancet 2002; 359: 1388-92)
Mediastinal staging withCT, PET, and endoscopic esophageal ultrasound (EUS) • EUS+FNA better ? for locoregionalstaging (N) • PET wassuperior (highersensitivity and specificity), to CT but also to EUS. • [Chest 2003;123(suppl 1):137S–146S]. • PET and EUS withfine-needle aspiration had similarsensitivities (79%) for advanced cancer, but EUS with FNA had a superiorspecificity (100% vs. 72%). • [Am J RespirCritCare Med 2003;168:1293–1297] • EUS withfine-needle aspiration had highersensitivity (87% vs. 61%), specificity (100% vs. 91) and accuracy (94% vs. 77%) than PET. • [ClinGastroenterolHepatol 2006;4:846-51]. • In 5 papers on > 300 patients with PET positive N (N1-3): EUS+FNA had high accuracy and in ~50% detected malignancy obviating the need for further surgical procedures • [Chest 2005;128:3004-9 & 2005;127:130-7][Ann Thorac Surg 2005;80:1231-40][Thorax 2004;59:596-601][Lung Cancer 2004;44:59-60].
Mediastinal staging withCT, PET, and endobronchial ultrasound (EBUS) with TBNA • 102 patients with potentially operable suspected lung cancer. • Gold standard: histology-cytology [Chest 2006;130:710-718]. • EBUS with TBNA vs. PET vs. CT: • Sensitivity (92% vs. 80% vs. 77%), • Specificity (100% vs. 70% vs. 55%), • Accuracy (98% vs. 73% vs. 61%). • EBUS + TBNA better ? for locoregional staging (N) In the majority of 33 patients with PET positive N (N1-3): EBUS-TBNA could detect malignancy obviating the need for futher surgical procedures [Eur Respir J 2006;27:276-281].
PET/CT improves staging in lung cancer ”PET/CT improves staging in 20-40% of lung cancer patients compared to PET and CT” (T and N status) Lardinois D et al. N Engl J Med 2003;348:2500-7 “Compared to PET, PET/CT better predicts stage I and II, as well as T and N status” Cerfolio RJ et al. Ann Thorac Surg 2004; 78: 1017–23 ”PET/CT is significantly better than CT in NSCLC staging and provides enhanced accuracy and specificity in nodal staging” (10 FN Nodes with CT and 5 with PET/CT) Shim SS et al. Radiology 2005; 236:1011-9 ”PET-CT is more accurate, sensitive and specific compared to CT alone in nodal staging. Nael Al-Sarraf et al. Lung Cancer 2008;60:62-8 PET/CT 10-15% more accurate than PET
Extrathoracic metastasis • 40% with NSCLC have distantmetastases at presentation, most often in the • adrenal glands,bones, liver, or brain [Ann Thorac Surg 1996;62:246–250]. • Adrenal glands: 10% of NSCLC have enlarged adrenal glands on CT, 2/3 being benign. • PET has high sensitivity (100%) and specificity (80%–100%) -> reduces number of unnecessary adrenal biopsies. • Bone: Bone scintigraphy good sensitivity (90%), low specificity (±60%), PET similar or higher sensitivity (90%), similar or higher specificity ( 98%),and higher accuracy (96%). • Liver: US and/or CT and /or MR remain thestandard imaging techniques for the liver. No good comparisons studies. Additional diagnosticinformation by PET combined with CT, in thedifferentiation of hepatic lesions that are indeterminate onconventional imaging. • Brain: FDG-PET low sensitivity (60%) not suited for the detection of brain metastases. The Oncologist 2004; 9 (6): 633-43; (Lung Cancer 2004;44,317-25)
True positive FDG-PET in spine, false negative bone scan at presentation, but true positive 3 months later Lung Cancer (2004) 44, 317—325
Diagnostic value of PET in lung cancer Solitary pulmonary nodules (SPN) Mediastinal staging (N) • Sensitivity ~ 97 % (SPN); ~ 73% (N staging) • Specificity ~ 78 % (SPN), ~ 93% (N staging) • Reasons for false negative ? • Reasons for false positive ?
Value of PET in lung cancer • Reasons for false negative • Small size (resolution 4-6 mm, respiratory movement) • Well-differentiated tumors: • Some bronchioalveolar carcinoma (GGO) • Some carcinoids (Neuroendocrine tumors) • E.g. Adenocarcinoma • E.g. Renal cell carcinoma
Pitfalls of FDG-PET in lung cancer False positive • Inflammation • Granulomas: • Tuberculosis • Sarcoidosis • Histoplasmosis • Silicosis • BOOP, etc. • Iatrogenic causes • Invasive procedures • Talc pleurodesis • Radiation sequelae • Focal physiological FDG uptake • Gastrointestinal tract • Striated muscles • Brown fat • Artheroschlerotic plaques TB in a 58-year-old man. (A) chest radiograph shows two nodules (b) coronal FDG PET scan shows increased uptake (solid arrow) in the left upper lobe nodules (SUV 4). Radiology 2000 6:117-21 Fischer BM, Mortensen J. Respiration 2006;73:267-76
Sarcoidosis Monitoring: Localisation of activity in- and outside lungs: Before treatment: After inhaled steroid: After prednisolone: • Milman N, Mortensen J, Sloth C. Respiration. 2003;70:408-13. Indication for use of PET
Guidelines • PET/CT is now implemented in guidelines
PET & PET/CT in guidelines for staginglung cancer to improvestaging(Nodes+Metastases) & avoidunneccesarysurgery ESTS guidelines for preoperativelymph node staging in NSCLC Eur J Cardio-thoracicSurgery 2007; 32:1-8 Noninvasive Staging of Non-small Cell Lung Cancer* ACCP Evidenced-Based Clinical Practice Guidelines (2nd Edition) Silvestri, G. A. et al. Chest 2007;132:178S-201S The Danish National Board of Health, 18 jan 2008: PET/CT in lung cancer staging for potentiallycurable patients
STAGING OF NSCLC ESTS-guidelines Invasive procedures can be omitted in patients with peripheral tumors and negative mediastinal PET (N0) In case of central tumors, PET hilar N1 disease, low SUV of primary tumor and LNs 16mm on CT, invasive staging remains indicated. PET positive mediastinal findings should always be confirmed cyto-histologically. so staging remains indicated. De Leyn et al. Eur J Card-Thor Sur 2007;32:1-8
Newer indications for PET in lung cancer • PET predicts survival • SUV median survival • < 10 2 yr • > 10 1 yr • + mass >3 cm ½ yr • Ahuja et al. Cancer 1998; 83 ; 918-24 • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging Mesothelioma • In multivariate analysis,the SUV was independently predictive of disease-free and overallsurvival • Vansteenkiste J, Fischer BM, Dooms C, Mortensen J. Lancet Oncol 2004; 5: 531–40
Newer indications for PET in lung cancer • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging Mesothelioma • Re-staging after neoadjuvant therapy (invasive best) • Early assessment (Reduction in metabolism correletes closely to outcome) • Re-staging after completion of therapy (scar/residual tumor) Vansteenkiste J, Fischer BM, Dooms C, Mortensen J. Lancet Oncol 2004;5:531-40
Newer indications for PET in lung cancer • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging Mesothelioma • PET/CT guided RT improves radiation dose to the tumor • and metastases and reduce dose to adjacent normal tissue • Target volumes in NSCLC were changed by PET/CT: • Several studies show changes between 35-62 % (Increased and decreased) • No studies with patient outcome yet
Newer indications for PET in lung cancer • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging (and monitoring) SCLC CT/Bone scint/bone marrow PET PET/CT Sensitivity 79% 93% 93% Specificity 100% 83% 100% PET/CT (n=32) changed stage in 17% of SCLC (LD->ED in 10%) “PET/CT can simplify and perhaps even improve the accuracy of the current staging procedure”. Fischer MBB, Mortensen J et al. Ann Oncol 2007;18(2):338-45 Brink et al (PET only, n=120) Significantly superior to CT in the detection of distant metastases: PET changed stage in 12% (upstaging 10, downstaging 3 of 120)
Newer indications for PET in lung cancer • Prognostic information from SUV • Evaluation of treatment effect -> • PET/CT for planning of radiation field • Staging and monitoring SCLC -> • Staging Mesothelioma J Nucl Med. 1999 Aug;40(8):1241-5. Semin Oncol. 2002 Feb;29(1):26-35 Lung cancer 2005;49:s27-s32 J Thoracic Cardiovasl Surg 2005;129:1364-1370 • PET/CT for: • Extent of tumour and invasion? • Preop. staging extrathoracic/contralat. metastasis (not N1,2) • Monitoring treatment • Prognosis (high metabolism -> bad prognosis)
Conclusion • Diagnosis of SPN • Differentiate between benign/malignant SPN, unable to be biopsied • High negative predictive value • the uptake (metabolism) is an independent prognostic factor (high->bad prognosis) • PET of value as adjunct to low-dose CT lung cancer screening • Staging PET/CT improves conventional staging (CT+US+bone scintigraphy) • PET/CT changes stage and treatment in 10-50 % of patients • Usually a higher stage is found • Avoids unneccesary thoracotomy (in 10-20%) due to N2-3 or M disease • Mediastinoscopy may be avoided if PET/CT is normal in the Mediastinum (non-central T), but needs to be performed if PET/CT is positive • Emerging indications: • restaging • treatment monitoring, • radiation field planning, • staging SCLC and Mesothelioma
Simplify the staging procedure one-stop procedure More often assign the correct stage And correct treatment to the patient Better assesment of prognosis Therapy evaluation Other PET tracers eg. hypoxia tracers especially for RT Perspectives for PET/CT in lung cancer
Respiration gated PET (4-D PET) 12 mm solid nodule in R3; 89 d dobling time, PET positive, surgery T1N0M0 4-D PET Most relevant for peripheral basal nodules with much respiratory movement
Author Patients Design End Point Conclusion Van Tinteren et al. Lancet 2002; 359:1388-92 (PLUS study) 188 (9 centers) Pot. operable. Diagnosis in 50% 70% I+II Conv. vs. Conv.+PET 1 yr follow-up Med.scopy in 66% -PET, 73% + PET No. of Futile thoracotomies # (Cost) Rel. Reduction of 51% 41% (-PET) 21% (+PET) (Reduction in Cost) Herder et al. J Clin Oncol 2006;24(12):1800-6 465 (22 centers) 12-19 % benign 29-28 % I+II 9-11 % IIIa 33-32% IIIb+IV Conv. vs. PET up-front at first presentation. 1 yr follow up No. of non-invasive procedures for staging Cost and No. of non-invasive procedures similar, Rel. reduction in invasive procedures incl Med.scopies Viney et al. J Clin Oncol 2004; 22:2357-62 184 (4 centers) Pot. operable. Diagnosisin 100% 92% I, 8% II Conv. vs. Conv.+PET Surgeon decides to do (or not) med.scopy (in 10) and thoracotomy No. of total thoracotomies Slightly better staging with PET, No diff. in End Point. Management changed in 13% (+13%) Lassen U, Mortensen J, BMB Fischer, & DLCG et al. (closed) PERALUST study 220 (4 centers) Potent. operable. Conv. vs. Conv.+ PET/CT Med.scopy in 100% 1 yr follow-up No. of Futile thoracotomies # ? Data processing Randomised studies of PET in NSCLC staging