Download
1 / 65
660 likes | 812 Vues
The Cardiovascular system. Functions of the circulatory system. Transport Erythrocytes (red blood cells, RBC’s) carry oxygen from lungs, remove CO 2 from tissues Nutrients, hormones etc. all carried by the fluid portion of blood (NOT RBC’s)

E N D
Functions of the circulatory system • Transport • Erythrocytes (red blood cells, RBC’s) carry oxygen from lungs, remove CO2 from tissues • Nutrients, hormones etc. all carried by the fluid portion of blood (NOT RBC’s) • Metabolic wastes from body tissues delivered to renals • Protection • “White” cells (immune cells) • Antibodies, inflammatory mediators (cytokines), blood clotting factors • Regulation • Constant flow helps to stabilize fluid and fluid ingredient distribution (mixes everything equally) • Buffers pH changes in tissue • Buffers temperature changes
The heart • Two pump: Right (pulmonary system) and left pump (organ system) • Pumps 5 L/min (2.5+ million liters year, roughly 60-70 bpm, • An RBC takes 1 minute to travel from the heart to your finger or toe and back to the heart! • Roughly size of your fist
Heart - pericardium • Contained within pericardium • Parietal pericardium: • Outer dense fibrous connective tissue • Inner serous parietal pericardium • Visceral pericardium serous layer = epicardium • Produces serous fluid that surrounds heart proper
Heart – the wall • 3 layers form the heart “proper” (organ within the parietal pericardium) • Epicardium (visceral pericardium) • Where cardiac vasculature is located • Where you look for the root cause of damage during myocardial infarction • Myocardium (muscle layer) • Cardiac muscle cells • Arranged so that during contraction, chambers squeeze in a particular manner • Thickness reflects amount of force required to pump • Thickest in region of the Left Ventricle • Thinnest in the atrial walls • Endocardium (endothelium within the heart) • Inner lining of the heart chambers • Not very porous (acts as a “bag” to retain blood and prevent leakage between muscle layers)
Cardiac muscle • Most of your heart is made of cardiac muscle • Striated (like skeletal muscle in contractile protein arrangement) • Each cell is much shorter, and usually more thick as well • Each cell joined by an intercalated disc • An area of cell-cell adhesion, as well as a gap junction complex to permit 1 cell to stimulate the next
Cardiac muscle • Cardiac muscle cells have less developed sarcoplasmic reticulum • Less ability to store calcium • Have larger transverse tubules (the tunnels of the plasma membrane/sarcolemma) to permit extracellular calcium to enter more easily • Damage is repaired by fibrosis only • Reason why heart attack patients have such a hard time recovering…they’ve lost heart contractility and will never regain/repair it
Cardiac muscle • NO neural stimulus for contraction • Has “pacemaker cells” that set off rhythmic depolarizations (electrical pulses) to trigger your heartbeat • The autonomic nervous system feeds into these pacemaker cells to increase or decrease your heart rate, but these cells operate without neural control to make sure you heart ALWAYS beats • Known as “autorhythmic” because your heart does not need your brain to tell it to beat • These pace-maker cells are distinct from the cardiac muscle cells. They do not contract
Cardiac muscle • External heart structure: • Coronary sulcus: divides atria from ventricles • Think: “circumferential” or coronal plane sulcus • Interventricular sulci: divides left & right ventricles • Look for “adipose lines”
Cardiac muscle • External heart structure: • Various sulci serve as “routes” for cardiac blood vessels • Cardiac muscle reliant on cardiac blood vessels for blood supply (endocardium does not allow for much fluid or gas exchange within the heart)
Heart • Within the heart proper, 4 chambers & valves • Atria contract simultaneously, emptying into each respective ventricle • Atrial walls “reinforced” by pestinate muscles (gives the look of a wicker basket) • Interatrial septum = thin, muscular membrane separating left & right atria • Atrioventricular valves separate atria from ventricles • Ventricles = much more muscular (have to pump blood further) • Valves maintain one-way flow of blood through heart
Heart wall Within ventricles endocardium = specialized formation Trabeculae carnae: ridges & “mesh-like structure” within the ventricle to prevent “suction” If the inner wall of the ventricle were flat, as the ventricle contracted, it would have difficulty relaxing as the two flat surfaces would adhere together
The heart valves • Atrio-ventricular valves (A/V valves): separate atria from ventricles: • Right side: Tricuspid valve • Left side: Bicuspid or Mitral valve • Semi-lunar valves: • Pulmonary semi-lunar valve within the pulmonary trunk • Aortic semi-lunar valve, at the beginning of the aorta • The long cords, the chordae tendinae, hold the valves in place during contraction and prevent reflux
Coronary vessels Angiogram
Coronary arteries • Blood is brought to the cardiac muscle by the coronary arteries which originate at the base of the aorta: • Left coronary artery split into the circumflex artery and the left anterior descending (LAD) artery • The right coronary artery split into the marginal artery and the right posterior descending artery
Coronary veins • The blood from the cardiac muscle drains into the venous system. • It is collected by the Great cardiac vein, the small and middle cardiac veins. • The blood empties in the right atrium at the coronary sinus (not to be confuse with the S/A node or the pace-maker)
Heart Conduction • Conduction system create and spread a wave of depolarization. • This wave is then followed by cardiac muscle contraction • SA node = “pacemaker” due to cyclic depolarization of specialized neurons • Located in right atrium, near insertion of SVC • Depolarization spreads across BOTH atria • Recall both atria contract simultaneously • Impulse then passes down to atrioventricular node (AV node) • Inferior side of the interatrial septum atrioventricular bundle at most superior end of the interventricular septum L/R ventricles • In the ventricles, conduction fibers (Purkinje fibers) carry impulse throughout both ventricles
Heart conduction • This electrical activity sustained by the conduction system can be followed by the EKG (ECG) • The corresponding heart muscle contraction results in rhythmic contraction and movement of blood throughout the heart • See Human Physiology
“lub” “systole” “dub” “diastole”
Blood vessels • Tubular network for blood flow • Blood flow is a closed system (components of blood do not readily leave the blood vessels) • 3 layers to every blood vessel • Tunica externa (adventitia) • Most superficial layer of loose connective tissue • Tunica media • Smooth muscle layer • In arteries, tunica media layer contains large density of elastic fibers • Tunica interna (endothelium) • Simple squamous epithelial tissue with elastic fibers
Arteries Elastic fibers within the tunica media • Allows artery to expand when heart expels blood • Elastic fibers permit recoil to original shape following expulsion of blood from heart • Expansion & recoil (elasticity) acts to smooth out the blood flow (less pulsing) • As arteries reduce in size, they become less elastic • Small arteries, arterioles are less elastic than arteries • Capillary = 7-10 m diameter
Capillaries • Nutrient and gas exchanges are only possible across capillaries • Endothelium in arteries is quite “tight” • Over 40 billion capillaries in your body (1800+ square kilometers of coverage) • No cell is more than a few m from a capillary • Despite large surface area and extensive network, only 250 ml blood is within the entire capillary network at any one time! • Walls are unique • Simple squamous endothelium
Capillaries • 3 subtypes of capillaries: • Continuous capillary: tight pores between squamous cells • Muscle, lungs, adipose & CNS • Remember that in CNS, this is the basis for the blood-brain barrier…incredibly tight capillary network • Fenestrated capillary: fenestrations = windows/pores • Renals, endocrine organs & GI tract • Wide pores permits fast transfer of gas and nutrients/waste • Covered by a mucoprotein diffusion barrier • Discontinuous capillary: widest pore size • Bone marrow, liver & spleen • Pores so wide = sinusoids (sinus-like pores)
In discontinuous capillaries, the endothelial cells do not physically connect to one another. This permits pores so wide they’re called sinusoids. Discontinuous capillaries are restricted to organs that process LARGE volumes of blood
Veins • Carry blood from capillaries BACK to heart • From capillary – venule – vein • Very LOW pressure (0.02 psi) • Arteries can hold up to 5 psi (in some areas, even more) • At this low pressure, blood cannot return to the heart • Relies on 1-way valves (venous valves) and skeletal muscle contractions to propel blood back to heart • Only find valves in veins…never in arteries
Varicose veins = veins stretched from standing (stretched veins = pulled valves that don’t work correctly)
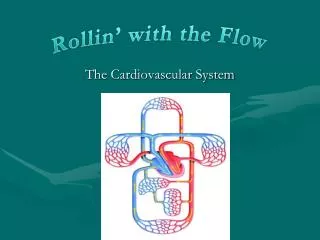
Circulation • Coronary circulation • Cardiac blood flow • Pulmonary circulation • Systemic circulation • Fetal circulation
Coronary circulation: blood circulation in myocardium • Ascending aorta aortic/semilunar valve L/R-coronary arteries • Left coronary artery anterior atrioventricular artery anterior region of both ventricles circumflex artery • Circumflex artery L-atrium & L-ventricle • Right coronary artery posterior interventricular sulcus Posterior region of both ventricles • From capillaries in myocardium cardiac veins • Anterior interventricular vein (drains from anterior region of heart) • Posterior interventricular vein (drains from posterior heart) • Merge into coronary sinus R-atrium Do not confuse coronary sinus and sinus atrial node or S/A node
Cardiac Blood Flow • L-atrium receives oxygenated blood from lungs via 2X right/left pulmonary veins • ONLY veins that carry oxygenated blood • The right atrium receives blood from the vena cavaes. • R and L-atrium contract and pump blood into the ventricles via the atrio-ventricular valves (A/V valves), the “bicuspid” or “mitral” for the left side and the tricuspid valve for the right side • Valve opening dependent upon ventricle RELAXATION • Ventricle contract & pumps blood into the systemic circulation: Through the aortic semilunar valve into ascending aorta on the left side and the pulmonary semi-lunar valve into the pulmonary trunk on the right side. 3 4
Cardiac contraction is systole. Cardiac relaxation is diastole. The atria relax blood flows min, passively. Both atria contract at the same time to force blood into the ventricles. Both ventricles then contract at the same time to propel blood towards the pulmonary artery or the aorta. “lub” “systole” “dub” “diastole”
Pulmonary circulation • Blood vessels that transfer blood between heart & lungs • Blood “vessel-way” • R-ventricle pulmonary valve pulmonary trunk L/R-pulmonary arteries pulmonary capillaries (in lungs) pulmonary veins L-atrium • Note how the coronary circulation begins at the right ventricle and ends at the left atrium
Systemic circulation • Everything OUTSIDE the pulmonary circulation • Includes the coronary circuit as well • From: • Left ventricle aortic valve ascending aorta systemic vasculature capillaries (not within the lungs) venous apparatus right atrium
Portal circulation • Portal circulation: vein-capillary-vein • Recall portal circulation in the adenohypophysis (anterior pituitary) • Carries venous blood from hypothalamus into the capillary bed of the adenohypophysis • Hepatic portal blood circuit • Drains blood from the gastrointestinal viscera via hepatic portal vein, into the liver (hepatic) system before emptying into the IVC via the hepatic vein
Principle Arteries Aorta = major systemic artery Aortic arch Directly from left ventricle = ascending aorta Right & left coronary arteries are the ONLY branches at this point Aortic ARCH Brachiocepalic trunk Further branches into right subclavian artery & right common carotid artery Next branch = Left common carotid artery Third branch = Left subclavian artery
Principle Arteries Towards upper appendage via subclavian artery Arterial blood from subclavian artery has a number of “choices” Vertebral artery = towards cranium via transverse foramen of the cervical vertebrae & enters cranium via foramen magnum Thyrocervical trunk = destined for thyroid Internal thoracic artery = destined for thymus & pericardium Costovertebral trunk = destined for intercostal muscles & spinal meninges
Principle Arteries Towards upper appendage via subclavian artery Arterial blood from subclavian artery has a number of “choices” If destined for the appendage: Subclavian artery = axillary artery between 1st rib & median edge of the humerus Past medial side of humerus = Brachial artery Around humerus = anterior & posterior humeral circumflex arteries Ring of arteries around humeral muscles Bifurcates into radial & ulnar arteries proximal to cubital fossa Radial = pulse at the wrist
Principle Veins From upper appendage In order to return arterial blood that has passed out of the capillary beds throughout the upper appendage: Combination of superficial & deep veins Superficial veins often quite variable in location Deep veins usually follow arteries Radial & ulnar veins draw blood from palmar region Both anastomize into brachial vein Superficial basilic vein draws blood ulnar & medial veins Eventually anastomize with brachial veinaxillary vein Superficial cephalic vein draws blood from superficial radial region of arm
Principle Veins From upper appendage Once all upper appendicular veins have anastomized into axillary vein: Axillary veinsubclavian vein Receives venous drainage from cranium as well External jugular vein (“external” skull) Internal jugular vein (brain, meninges etc.) Physically larger than external jugular Adjacent to common carotid artery Where internal jugular vein merges/anastomizes with subclavian vein = brachiocephalic vein
Principle Arteries Abdominal: 4 branches from the dorsal/descending/abdominal aorta Celiac trunk Splenic artery L-gastric artery Common hepatic artery Further bifurcates into gastroduodenal artery & “proper” hepatic artery Superior mesenteric artery Branches throughout mesentery (small intestine, upper 2/3 large intestine, pancreas) Left & right renal arteries Inferior mesenteric artery Branches throughout distal/terminal mesentery (termnal colon, rectum)