Download
1 / 37
390 likes | 943 Vues
Hand-Foot-Mouth Disease/ Enterovirus 71. Piyarat Suntarattiwong Queen Sirikit National Institute of Child Health. Enterovirus : viral classification. Hand-foot-mouth diseases. HFMD พบว่าเกิดจากเชื้อ Enterovirus serotype coxackie A16 มากที่สุด

E N D
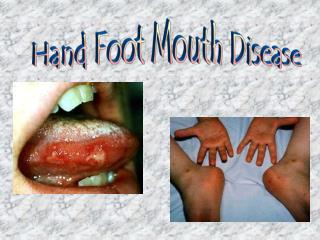
Hand-Foot-Mouth Disease/ Enterovirus 71 Piyarat Suntarattiwong Queen Sirikit National Institute of Child Health
Hand-foot-mouth diseases • HFMD พบว่าเกิดจากเชื้อ Enterovirus serotypecoxackie A16 มากที่สุด • รองลงมาคือ serotype enterovirus 71, coxackie A5,7,9 & 10, coxackie B2 &5
Enterovirus 71 (EV 71) & HFMD HFMDที่เกิดจาก EV 71 HFMD EV 71 • มีอาการทางสมอง • Brain stem encephalitis • Encephalitis • Aseptic meningitis
Enterovirus 71 (EV 71) & HFMD • HFMD ที่เกิดจากเชื้อซีโรไทพ์EV 71พบneurological diseaseร่วมด้วยมากกว่าserotypes อื่นๆ • มีรายงานการระบาดรุนแรงและมีผู้เสียชีวิตจากซีโรไทพ์EV 71 • Bulgaria 1975 – 44 deaths • Hungary 1978 – 45 deaths • Malaysia 1997 – 30 deaths • Taiwan 1998 – 78 deaths, 2000 – 25 & 2001 – 26 deaths • และมีรายงานการเสียชีวิตจากHFMD/EV 71 ในประเทศจีน สิงคโปร์ เกาหลี และออสเตรเลีย • ประเทศในเอเชียตะวันออกเฉียงใต้
การสอบสวนโรค HFMD ในไทย • 2001 (พ.ศ. 2544) : HFMD จัดเป็นโรคต้องรายงาน • ไข้และ • มีตุ่มหลายตุ่มขึ้นในปากและ • มีตุ่มพองใสขึ้นที่ฝ่ามือ ฝ่าเท้า และก้น • ข้อบ่งชี้ที่ต้องส่งตรวจยืนยัน และสอบสวนการระบาดคือ • มีความรุนแรงต้องนอนโรงพยาบาล หรือเสียชีวิต • มี HFMD เป็นกลุ่มในหมู่บ้านหรือในโรงเรียน หรือในสถานรับเลี้ยงเด็ก
HFMD caused by EV 71 at QSNICH in 2001(Viral isolation & serology) งานวิจัยโดยนพ. ทวี โชติพิทยสุนนท์ สถาบันสุขภาพเด็กแห่งชาติมหาราชินี
อาการทางคลินิกของการติดเชื้อ EV 71 • 80% แสดงอาการเป็นมือเท้าปาก ที่หายได้เอง(self-limiting HFMD, Herpangina, Febrile illness) • อาการรุนแรง • aseptic meningitis • encephalitis (brainstem encephalitis) • การอักเสบของก้านสมอง pons & medulla • encephalomyelitis • acute flaccid paralysis
การวินิจฉัยแยกโรคจาก Herpetic gingivostomatitis
อาการชนิดรุนแรงของผู้ป่วย EV 71 • อาการนำคือHFMD (68%) หรือherpangina(15%), อาเจียน, ไข้ เฉลี่ย 3 วันแล้วต่อด้วยอาการทางสมองได้แก่ • Aseptic meningitis • Polio-like paresis • Brain-stem encephalitis (90%) • Truncal ataxia, myoclonus, intention tremor • impaired consciousness • sudden cardiovascular collapse
ผู้ป่วยนำเสนอรายที่ 1 : รับไว้ในรพ. เด็ก กันยายน 2551 • เด็กชาย 1 ปี 3 เดือน • ไข้ อาเจียน ตุ่มขึ้นที่เท้าสองข้างมา 2 วัน • ซึ่งไม่ดีขึ้น (แย่ลง) หลังจากได้รับยาแก้ไข้ แก้คออักเสบ • รับไว้สังเกตอาการให้IV fluid ยาแก้ไข้และยาปฏิชีวนะชนิดฉีด • CBC: Hct 31.5% WC 18,750 (N 75, L 21, M 4) plt. 476,000 • อาการไม่ดีขึ้น ท้องอืด อาเจียน ซึม รับไว้ตึกผู้ป่วยใน
PE • T 39.5 P 104/min RR 42/min • BW 8.2 kg • HEENT: no intraoral lesion, injected pharynx • Heart: normal S1 S2 • Lung: clear • Abd: mild distention, liver & spleen – neg. • Extremity: a few small vesicles & MP rash both soles
Progression • 3hr after admission, he vomited many times • Lethargy • Develop dyspnea • BP 80/50 sat. 89% • Rales both lungs • He was intubated • +pink frothy sputum
He was on ventilator • Developed convulsion • Tachycardia HR 200-220/min • Developedhypotention • Inotropic drugs, IVIG were given • The patientdied after 14 hrs.
Specimen collection • Stool: PCR positive for EV 71 • Throat swab: negative for EV 71 & others HEV • Serum antibody • EV 71 = 1:1,536 • Cox A10 = 1:12 • A16 < 1:4 • No second serum
Perivascular cuffing Neuronophagia • BRAIN • Scattered foci of neuronal necrosis involving cerebellum, midbrain, pons, and spinal cord • - Diffuse pulmonary edema and hemorrhage, all lobes of both lungs
การยืนยันการวินิจฉัย • การวินิจฉัยทางคลินิก • การตรวจยืนยันเชื้อไวรัส • ระยะแรก:- น้ำจากตุ่ม และ/หรือ ป้ายในคอเจาะเลือดครั้งที่ 1 • ระยะหลัง 7 วัน:- อุจจาระ และเจาะเลือดครั้งที่ 2 • น้ำจากตุ่ม และ/หรือ ป้ายในคออุจจาระ: • หาเชื้อไวรัสด้วยการเพาะเชื้อไวรัส หรือ พีซีอาร์ • เลือด: • ดูการเพิ่มขึ้น 4 เท่าของระดับแอนติบอดี
Treatment of EV 71 • Immune globulin : • Humoral immune response (Neutralizing antibody) inhibit EV • Limited data – IVIG treatment • Antiviral drug: • Pleconaril – suspended by FDA
Guide to treatment and risk factors Modified from Chang LY et al. Lancet 1999
Stage II: Meningoencephalitis • Admit to PICU p.r.n. • Monitor BP, HR, sugar, ABG, e¯ ,coma scale • Intubate patient and provide mechanical ventilator for GCS< 9 or significant IICP or any deterioration signs • IVIG:1gm/kg • Fluid restriction: 1/2-2/3 maintenance • Furosemide for patients with high CVP?? • Invasive monitoring: CVP, ABP • Consult cardiologist as needed and arrange echocardiography
นำเสนอผู้ป่วย : รับไว้ในร.พ. เด็ก เดือนตุลาคม 2551 • เด็กชาย 1 ปี 2 เดือน • มีไข้ ไอ และอาเจียน 1 วันก่อนมารพ. • สงสัยหอบหืด (เคยหอบมา 1 ครั้ง) • PE: • T 39.5 ⁰c RR 36/min PR 120/min • Mild dehydration, injected pharynx & tonsils • Heart & Lungs: rhonchi • Abd: WNL • Neuro: stiff neck ѳ
Admission diagnosis:bronchitis • CBC: Hct 35% WC 23,000 (N85% L15%) Plt. 240,000 • IV antibiotics & supportive care • Progression: • D2 :ยังคงมีไข้ ไอ และดูซึมลง • มีตุ่มแดงขึ้นที่ขาทั้งสองข้าง • R/O Dengue fever– repeat CBC: normal platelet count • Follow VS:BP170-180/110-100 • 2 ชม. ถัดมา ผู้ป่วยเกิดอาการหอบเฉียบพลัน เขียว ซึมมาก ย้ายไอ ซี ยู
Treatment & Investigation • Respiratory support with HFV • Inotropic drugs • IVIG • CT brain: unremarkable • MRI: diffuse meningoencepahlitis with prominent encephalitis in the brain stem
Specimens • Stool – PCR +EV 71 • Tracheal suction & throat swab – PCR -EV 71 • His 3-y-old sister develop mildHFMD • The sister’s stool– PCR +EV 71
Serology • 1st serum: • Entero 71 1:6,144 • Cox A10 1: 4 • Cox A16 1: 4 • 2nd serum: • Entero 71 1:6,144 • Cox A10 1: 24 • Cox A16 1: 48
ผู้ป่วยอาการทุเลาก่อนจะให้กลับบ้านผู้ป่วยอาการทุเลาก่อนจะให้กลับบ้าน
EV 71 Viral testing & surveillance recommended in: • Severe HFMD need hospitalization • Complication : • Respiratory, Cardiovascular and Neurologic complication • Clusters of HFMD • Acute pulmonary edema of unidentified cause
Specimen collection • 8 grams of stool in the sterile tube • Put in the sealed plastic bag • Keep cold (ice packs) • PCR • Throat swab( symptoms <7 days) • PCR • Paired serum-14 days apart • Antibody- microneutralization test
Control measure • Isolation • Contact (fecal-oral route) • Young children are susceptible • Nursery, kindergarten, elementary school • A Classroom closure:2 cases of HFMD ina class • A school closure: >1 class or > 5 cases • For 7 days: (5 working days) www.ddc.moph.go.th