Download
1 / 14

E N D
“The weak can never forgive. forgiveness is the attribute of the strong.” – MK Gandhi
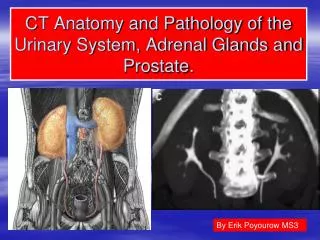
Shashidhar Venkatesh Murthy A/Prof & Head of Pathology College of Medicine & Dentistry CLINICAL PATHOLOGY The foundation of clinical medicine. BPH3: Urinary Tract Dis: Prostate, BPH
3 Male Urogenital System: Prostate Periurethral, Fibromuscluar gland. Function – Semen, acid phosphatase. Sperm nutrition. Hormone response – Androgens, Testosterone. Prostatitis, BPH & Cancer. Central Zone - BPH Peripheral zone - Cancer
Prostate: Zones Trans. Zone BPH BPH Anterior Posterior
5 Normal Prostate Histology: Fibromuscular gland. 1. Fibromuscular stroma 2. Glands double layer epithelium. 3. Secretions (corpora amylaceae)
6 Prostate: Pathology Disorders of Prostate: 1. Inflammations – infections - Prostatitis 2. Benign Prostatic Hyperplasia* 3. Neoplasms – Prostatic Carcinoma* BPH Cancer
7 Prostatitis: Inflammation, edema, rectal pain, obstruction/dysuria. Acute suppurative prostatitis 5% E.coli, rarely Staph or N. gonorrhoeae Chronic non bacterial / chronic pelvic pain sy. 90% Chronic Inflam, symptoms, no pathogens. Asymptomatic inflammatory prostatitis. Only WBC, no symptoms no pathogens. Granulomatous prostatitis BPH, infarction, post TURP, idiopathic, TB, or allergic(eosinophilic). Diagnosis: Fluid examination after prostatic massage. Needle aspiration study of prostatic tissue.
One single grateful thought raised to heaven is the most perfect prayer. G. E. Lessing German critic & dramatist (1729 - 1781)
9 BPH-Introduction Non-neoplastic, androgen hyperplasia. Castration no BPH Testosterone DHT Hyperplasia. Common, 75% of men 70-80years. Only few symptomatic. Involves periurethral transitional zone. Morphology: Nodular hyperplasia of glands & stroma. (like in breast, thyroid etc) Stromal & Gland hyperplasia. Cystic glands, secretions, double layer maintained. BPH is NOT a precursor to carcinoma!
10 BPH: Morphology: Gross & Microscopy Gross: Grey white, nodular Hyperplasia, Periurethral zone. Microscopy: Hyperplastic cystic glands. Normal double layer epithelium
11 BPH: Complications Enlarged prostate. Median lobe - ball valve** 1. Urinary Obstruction 2. Urine retention 3. Inflammation / infections 4. Hypertrophy of wall 5. Mucosal trabeculations 6. Urolithiasis – stones. Stone
12 BPH: TURP (Diagnosis + Treat ) Trans Urethral Resection of Prostate Complications: Hemorrhage, Infection, Granulomatous prostatitis Retrograde ejaculation.
13 Normal Prostatitis BPH – –
“The only gracious way to accept an insult is to ignore it. If you can’t ignore it, top it. If you can’t top it, laugh at it. If you can’t laugh at it, it’s probably deserved...!” - - Joseph Russell Lynes