Download
1 / 34
350 likes | 574 Vues
Medical Theraphy of Idiopathic OAT. Hyun-Joo Kim M.D. Department of Urology Pochon CHA University. Medical Theraphy of Idiopathic OAT. Current Treatment Modalities Considerations Mission. OAT as a Diagnosis?. Concept of OAT ≒ FEVER OAT is a Phenomenon !.

E N D
Medical Theraphy of Idiopathic OAT Hyun-Joo Kim M.D. Department of Urology Pochon CHA University
Medical Theraphy of Idiopathic OAT • Current Treatment Modalities • Considerations • Mission
OAT as a Diagnosis? Concept of OAT ≒ FEVER OAT is a Phenomenon !
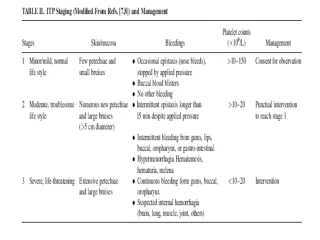
Criteria of OAT on Semen Analysis Oligospermia <20x106/ml (WHO) severe <5x106/ml crypto <1x106/ml a few motile or immotile Astheno <50% (WHO) severe <10% Terato <30% (WHO) <14% (Strict Criteria) severe < 4% (Strict Criteria)
Idiopathic v.s Specific • Specific Causes • Secondary Hypogonadism • Varicocele • Retrograde Ejaculation • Infections • Immunologic Infertility • Idiopathic Causes • All unknown causes
Prevalence of Male Infertility Normal/OAT 84.3% Azoospermia 15.7%a Obstructive 6.3%b Non-obstructive 9.4%c a. 981/6242 semen analysis (95.9-97) b. 165/416 testis bx (95.9-97) c. 251/416 testis bx (95.9-97)from CHA
Prevalence of Abnormal Semen Parameters • All parameter 43% • Motility 39% • Oligospermia 10% • Morphology 8% from Greenberg, 1987
Specific Causes v.s Idiopathic • Varicocele 39% • Obstructive 8% • Mechanical 8% • Endocrine 6% • Developmental 5% • Immunologic 1% • Idiopathic 33% from Schlegel and Pavlovich, 1997
Current Management Modality of Idiopathic OAT • Pharmacological • Sperm processing • ART
Management Idiopathic OAT: Pharmacological Treatment • Hormonal Treatment • GnRH • HCG/HMG • Purified or recombinant FSH • Androgens • Anti-Estrogens • Non-Hormonal Treatment • Kallikrein • Bromocriptine • Anti-Oxidant: Vit. C or E
Meta-Analysis of Medical Treatment in OAT Antiestrogens n=459 FSH n=223 Androgens n=1025 Kinin enhancing agents n=197 odds ratio
Role of FSH ( in Monkey) Normal Normal + FSH Hypophysectomy + T Hypophysectomy + T + FSH
FSH on Spermatogenesis I • Quantitative Influence • Increase A-pale spermatogonia Spermatocyte, Spermatid • Qualititative Influence • Restore defective spermatozoal maturation (esp. acrosomal cap) • For adequate concentration of intratubular Testosterone • LH for T, FSH for ABP
FSH on Spermatogenesis II • Stimulate Sertoli cell to enhance FSH dependent functions • Support spermatogenesis without interfering negatively with Leydig cell physiology and without locally increasing Estrogen level • Modulate intra-testicular paracrine and autocrine mechanism
Variable Results of FSH Treatment • Dose: may not high enough • Frequency : short half-life • Duration : too short • Reduction in FSH receptor activity • Low proliferative activity of A-pale spermatogonia • Elevated endogenous level of FSH
Management Plan for Idiopathic OAT I • Considerations: Female factor, Severity of OAT, Previous Treatment, P/E • Oligo: • T.Vol.(normal), FF(-): Empirical Tx > 3mos. • T.Vol.<10cc or FF(+): ART • Severe OAT: ART • A few motile/immotile: ICSI p.r.n) oocyte freezing • Astheno: • >10%, FF(-): Empirical Tx > 3mos. or IUI • <10%, FF(-): Empirical Tx > 3mos. or ICSI p.r.n) T-Bx • 0%: Vital >20-30% : ICSI Vital <10% : TESE-culture
Management Plan for Idiopathic OAT II • Terato: • General condition control • Empirical Tx > 3mos. + IUI • Severe Terato: • General condition control • Empirical Tx > 3mos. p.r.n) IUI or ICSI • FF(+): ICSI
Treatment of Male Infertility? • Relative Concept of FERTILITY • Consider Cumulative P.R • Natural Pregnancy or ART?
Cumulative Live Birth Rate 52.5%/36mos. 25.2%/36mos. From Kamischke, 1999
Male Fecundity from Schrader, 1988 Intra-and inter-individual variation of semen parameters in human, coefficient of variation
Drugs, Chemical, and Metabolites possible to exert toxic actions on the male gonad Parent compound Usage Metabolites Amiodarone anti-arrhythmia Desethylamiodarone Cephalosporin analogues anti-microbial drug N-Methyltetrazolethiol Valproic acid anti-epileptic drug Isomers of 2-ethyl hexanol(?) Diethylhexyl phthalate plasticizer Mono-ethylhexylphthalate (MEHP) (DEHP) 2-ethyl hexanol(?) Dibromochloropropane fungicide Dichloropropene derivatives (?) (DBCP) Ethylene glycol industrial solvent 2-Methoxyacetaldehyde (MALD) monoethyl ether n-Hexane environmental toxicant 2,5-Hexanedione Acrylamide industrial use N-Methylacrylamide, N-isopropylacrylamide Vinclozolin fungicide Butenoic acid derivatives enanilide metabolite 1. Only substituent is a testicular toxin, not cephalosporin 2. Questionable testicular toxin but probably teratogenic fromThomas, 1996
Environmental/Lifestyle factors to affect male fertility • Cigarette smoke • Ingestion of female sex hormones • Exposure to heavy metals(i.e. lead, arsenic) • Alcohol • Marijuana, anabolic steroids, cocaine • Cancer chemotherapeutics • Radiation exposure • Increased testicular temperature • Stress • Lack of exercise • Caffeine
Causes of Male Infertility • Pre-Testicular • Disorders of H-P-G axis • Testicular • Spermatogenic Defects • Post-Testicular • Epididymal Dysfunction • Obstructive change of passage • Infection of Accessary glands
Prevalence of Male Infertility • Pre-Testicular 8% • Testicular 80% (Idiopathic > 25%) • Post-Testicular 12% from Sigman, 1987
Testicular Causes: Spermatogenic Defects • Germ cell Defects • Somatic cell Defects • Communications Defects
Testicular expression of cytokines Cytokines Production Receptor Leydig cell Sertoli cell Germ cells IL-1 L, S,G + + + IL-6 L, S, + + ? TNFa G ? + ? IFN P,S,G n n n c-kit ligand S + n + EGF/TGFa L,P,S,G + + + TGFb P,S + + + Activin L,P,S + + + Inhibin L, S + + + IGF-I L,P,S,G + + + FGF L,P,S,G + + + NGF G n + - PDGF L, S + + -
Function of Testis • Dependent on Gonadotropins and Correct action of local growth factors • Major system • Endocrine System • Local factors • depend on Endocrine system • “act as an adjusted fine local relay for the endocrine system”
Spermatogenic Defects OAT from • Inadequate Gonadotropin activity • Imbalance in the intratesticular paracrine regulation • Mystery
Possible Diagnostic Tools of Spermatogenic Defects • Sperm chromosomal study • Gonadotropin assay • Germ cell and Somatic cell activity study • Receptors study
Medical Treatment of idiopathic OAT For the good results of treatment, Pt. SELECTION by Correct Diagnosis is mandatory!