Final Case Study
Final Case Study . Case # 4 Nancy Lee, Andrea Ustarez, Luis Castellon CSULA. Case Summary.

Final Case Study
E N D
Presentation Transcript
Final Case Study Case # 4 Nancy Lee, Andrea Ustarez, Luis Castellon CSULA
Case Summary • A 3-year-old girl was diagnosed with pneumonia, caused by Streptococcus pneumoniae. She had fever, high respiratory rate, and low blood oxygen saturation. Her lymph nodes were enlarged and a chest X-ray showed diffused consolidation of the lower lobe of the left lung. • She had pneumonia before, when she was 25 months old. She also had 10 episodes of otitis media that required antibiotic treatment. • Her immunoglobulin levels were measured: high levels of IgM, undetectable levels of IgA, and low levels of IgG. • She was previously vaccinated against tetanus and Haemophilus influenzae, but she did not express specific IgG against the tetanus toxoid or the polyribosyl phosphate (PAP) polysaccharide antigen of H. influenzae. • She had blood type A so she was tested for anti- antibodies. Her IgM titer of anti-B antibodies was positive at the upper limit of normal, her IgG titer was undetectable. • Her peripheral blood lymphocytes were analyzed showing normal expression of CD40 ligand on T cells activated by anti-CD3 antibodies, and normal expression of CD40 on B cells. Her blood cells completely failed to secrete IgG and IgE after stimulation with anti-CD40 antibody (to mimic the effects of engagement of CD40 ligand) and interleukin4 (IL-4).
Key Information Pointing to Diagnosis CLINICAL Features • 3 years old • Recurrent infections • Pneumonia 25 mo ago • 10 episodes of otitis media • Streptococcus pneumonia found in blood • Enlarged lymph nodes in neck and armpits LABORATORY Features • High IgM 470 mg/dl (normal 40-240 mg/dl) • Low IgG 40 mg/dl (normal 639-1344 mg/dl) • Undetectable IgA • Upon vaccination no specific IgG antibodies • Treatment w intravenous antibiotic showed improvement • Failure to secrete IgG and IgE after stimulation • Normal expression of: • CD40 L on T cells • CD40 on B cells
The Diagnosis for Case # 4 HIGM2 - Hyper IgM syndrome type 2 (AID deficiency).
Diagnostic Tests for Activation-induced Cytidine Deaminase (AID) Deficiency • Complete physical examination. • enlarged lymph nodes (sign of lymph node hyperplasia) • Immunohistological Examination Lymph Nodes. • follicular hyperplasia and enlarged germinal centers • Complete blood count (CBC) and Measurement of serum immunoglobulin levels • Elevated level of IgM, and diminished serum IgG and IgA levels • Flow cytometry • normal expression of CD40 and CD40 ligand • Molecular Genetic Testing: • DNA Analysis for AID mutations of autosomal recessive gene of consanguineous (related by blood) families • Analysis of CD40 ligand, CD40, Uracyl N-glycosylase to confirm the deficiency and rule out other possible causes.
Therapy for HIGM2 • Regular infusions of IVIG (400-600 mg/kg every 2 to 3 weeks or monthly). • IgG collected from 100’s-1000’s of individuals, filtered and purified, given intravenously in equal doses over 2-5 consecutive days. • HIGM2 is characterized by not showing opportunistic infections, so no prophylaxis is needed unlike in other subtypes of HIGM.
Prognosis for AID Deficiency Hyper IgM syndrome • Fairly good, compared to other types of hyper IgM syndrome. • Rare disease: affects only 1: 2,000,000 births/year • Most children can continue to live normal, healthy lives and socialize despite this chronic disorder • provided that they receive adequate treatment/therapy and appropriate treatment for infections. • Changes in lifestyle that affects the entire family will be made though: • Frequent visits to doctors, specialists for regular assessments to look out for signs of long term damage to organs. • Lifelong immunoglobulin replacement therapy • Antibiotics to protect and prevent from further infections that the immunoglobulin treatment is not effective against • Extra care and protective measures in all environments, especially socially active environments
How would you communicate diagnosis and disease to the patient • Mrs. Tudor, after evaluation of your daughters symptoms and laboratory exams we have diagnosed her with AID deficiency. This condition is due to an inherited gene mutation that affects your daughters immune response. She is unable to make different antibodies, which help her body fight off infections, and that is why she gets sick so often. In order to help her body gain better immunity we can treat her using intravenous immunoglobulin therapy. This therapy involves injecting immunoglobulin into her blood. Some common side effects of this therapy include headaches, nausea, fever, malaise. Although not very common, side effects can also include anaphylactic reactions, aseptic meningitis, acute renal failure, stroke, myocardial infarction. However the therapy will provide your daughters body with the antibodies she is missing, and help her fight off infections.
Theoretical Immunological Basis • AID deficiency prevents isotype switch (immunoglobulin class switch). • After the B cell is activated, AID is transcribed and translated. • At the same time, transcription of the constant region of the DNA coding for Ig’s is taking place. • The isotype switch regions are cytidine-rich, as they are being transcribed, AID converts cytidine to uridine. • Uridine is not a base found in normal DNA and it is extracted by uracil-DNA glycosylase. • The damaged DNA is recognized by DNA repair endonuclease, which reattaches two different switch sites.
Theoretical Immunological Basis • AID deficiency also prevents somatic hypermutations – point mutations in the variable region of Ig. • These mutations alter the affinity of the antibody for its antigen • Reduced antigen binding leads to negative selection and cell death • Improved antigen binding leads to positive selection, proliferation and finally plasma cell development • These B cells cannot undergo affinity maturation after they are activated, they only proliferate. • IgM+ B cells start to accumulate in lymphoid tissue, producing an enlarged spleen and lymph nodes.
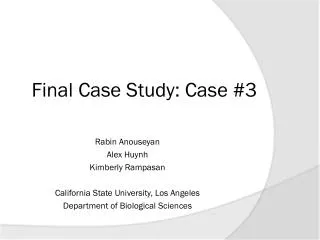
Activation-Induced Cytidine Deaminase (AID) Deficiency Causes the Autosomal Recessive Form of the Hyper-IgM Syndrome (HIGM2). • Revy et. al (2000). Cell. • Research objectives: To test the genetic basis of the HIGM2 syndrome and whether the human AID gene defects could cause the HIGM2 syndrome • Experimental set up: Identification of genetic basis for HIgM2 syndrome by performing a genome-wide search for susceptibility loci using polymorphic microsatellite markers in consanguineous families. They studied 18 HIGM2 patients from 12 families who fulfilled the diagnostic criteria of HIGM2. Performed Immunological Study of B cells, Linkage Analysis, HuAID Gene sequencing, HuAID Gene expression study, Cloning and sequencing of V3-23-Cµ Transcripts, Immunopathology of Lymph Nodes and Tonsils. • What did they find: Widely scattered point mutations in huAID are all defective. clearly demonstrate a crucial role of AID in Ig switch, Ig variable region gene somatic mutation generation, and normal germinal center formation. The possible candidate gene, human AID (huAID) gene has a strong linkage and maps to chromosome 12p13.
(B) Localization of mutations in the huAID gene. Nine different mutations were found in the coding sequence (red) in 18 patients tested. Mutations in patients P1-P2-P3, P4-P5, and P16 were localized in the cytidine deaminase catalytic region. In patients P1-P2-P3, a further heterozygous deletion was detected by Southern blot (not shown). Figure 2. Localization and Genetic Analysis of huAID Mutations in HIGM2 Patients
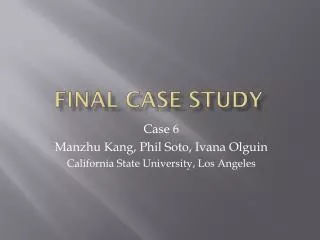
Figure 4. Immunohistological Examination of Cervical Lymph Node compared to control reactive lymph node from Patient P4 HE = hematoxilin-eosin staining (magnification ×25). P4 lymph node shows follicular hyperplasia with giant GC, compared with classical follicular hyperplasia, as control, shown at the same magnification.
Take Home Messages • AID deficiency involves a mutation in the AICD gene, which affects the ability of B cells to go through somatic recombination and class switching of immunoglobulin isotypes • Typical symptoms are enlarged lymph nodes, recurrent infections affecting the upper respiratory tract, GI tract and ears, high IgM, low IgG and IgA. • Diagnostic exams include examination of lymphoid organs, complete blood count to determine IgM, IgG and IgA concentrations in serum and molecular genetic testing. • Therapy is based on replacement of plasma by intravenous immunoglobulin therapy • Prognosis is fairly good, children diagnosed AID deficiency live a normal healthy life well into adulthood long as therapy is continued and infections are well treated.