LEUKEMIA IN CHILDREN
510 likes | 676 Vues
LEUKEMIA IN CHILDREN. Epidemiology. Approximately 2,800 children are diagnosed with ALL in the United States annually. It has a striking peak incidence between 2–6 yr of age and occurs slightly more frequently in boys than in girls. Introduction.

LEUKEMIA IN CHILDREN
E N D
Presentation Transcript
Epidemiology. Approximately 2,800 children are diagnosed with ALL in the United States annually. It has a striking peak incidence between 2–6 yr of age and occurs slightly more frequently in boys than in girls.
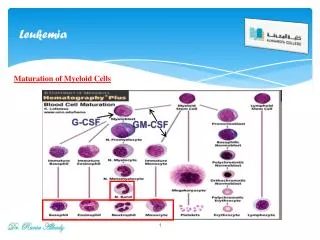
Introduction • Leukemia– the most common malignancy in childhood. • Acute leukemia– 97% Acute lymphoblastic leukemia– 75% Acute myeloblastic leukemia– 20% • Chronic leukemia– 3% Chronic myelogenous leukemia (Ph positive) Juvenile myelomonocytic leukemia ( JMML)
Leukemia • The most common childhood cancer ( 1/3 of pediatric malignancies ). • Acute lymphoblastic leukemia (ALL) represents about 75 % (peak incidence at age 4 years). • Acute myeloid leukemia (AML) accounts for about 20 % of leukemia (stable from birth through age 10) • Others : CML
Acute Lymphoblastic Leukemia • In the United States, about 3,000 children each year are found to have ALL • Peak incidence occurs from 3 to 5 years of age.
Acute Lymphoblastic Leukemia • the most common symptoms of leukemia:fever, anemia, bleeding and/or bruising, reccurent infections ,persistant weakness or tiredness, • achiness in the bones or joints, difficulty breathing (dyspnea) , adenohepatosplenomegaly
Clinical manifestations • Bone marrow failure & Organ infiltration • Common symptoms Fever ( 60%) Malaise ( 50%) Pallor ( 40%)
Etiology • Unknown( usually) • Hereditary Down’s syndrome Leukemia in siblings • Chemicals Chronic benzene exposure Alkylating agents • Ionizing radiation • Predisposing hematological disease ( MPD, AA) • Viruses ( HTLV-1)
Diagnostic criteria • ALL is often difficult to diagnose. • The early signs may be similar to the flu or other common diseases.
Diagnostic criteria • bone marrow aspiration and biopsy • complete blood count (CBC) • additional blood tests, genetic, molecular tests • computerized tomography scan • magnetic resonance imaging (MRI) • x-ray • ultrasound • lymph node biopsy • spinal tap/lumbar puncture
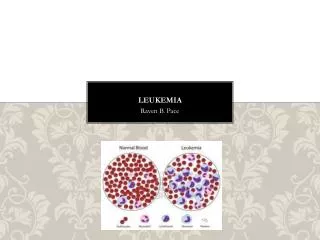
Diagnostic criteria • Peripheralblood: anemia,thrombocytopenia, variable white cell count with or without blasts. • Bonemarrow: hyper-or hypo-cellularity with excess of blasts (blasts>30% of nucleated cells).
Diagnostic criteria • Cytochemistry study and surface marker study confirm the lymphoid origin .
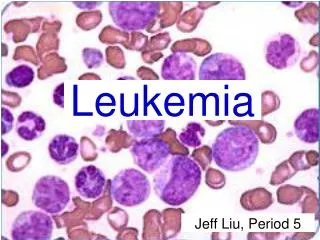
V-25Leukemic cells in acutelymphoblasticleukemia characterized by round or convoluted nuclei, high nuclear/cytoplasmic ratio and absence of cytoplasmic graulnes.
Differential diagnosis • AML. • MDS. • Non-Hodgkin‘s lymphoma with bone marrow involvement or with leukemic change. • Aplastic anemia • HIV infections • EBV • CMV • Systemic form of juvenile chronic arthritis
Laboratory examinations • Full blood count • Coagulation screening – especially AML M3. • Biochemical screening • Chest radiography • Bone marrow aspiration • Immunophenotyping • Cytogenetics & molecular studies • Lumbar puncture ( CNS involvement)
Complications • Cerebral hemorrhage, pulmonary hemorrhage or other vital organ hemorrhage. • Infection(sepsis or septic shock ) , pulmonary edema. • Tumor lysis syndrome. • Hyper K • HyperPo4). • Coagulopathy before or after chemotherapy. • Anemia.
Risk Grouping of TPOG (ALL) • Standard Risk • High Risk– CNS leukemia, cranial nerve palsy, testicular leukemia, pre-B ALL t(1;19) or E2A-PBX1 fusion
Very High Risk • WBC > 100000/mm3 • T – cell • < 1y/o • Lymphoblastic lymphoma with bone marrow lymphoblasts > 25% • t(9;22) or BCR-ABL fusion • t(4;11) or MLL-AF4 fusion • Other MLL gene rearrangement • Hypodiploidy ( chr 44 or less)
Poor Prognosis (I) • Acute lymphoblastic leukemia
Relapse • Bone marrow– the most common site, blast cell increase • CNS– IICP ( vomiting, headache, papilledema, lethargy) Convulsion Behavior disturbance • Testis– painless swelling
Survival rates • 75 % to 80% of children with ALL survive at least 5 years from diagnosis with current treatments that incorporate systemic therapy (e.g., combination chemotherapy) and specific central nervous system (CNS) preventive therapy (i.e., intrathecal chemotherapy with or without cranial irradiation).
Treatment • Chemotherapy– reach to remission(blast<5%) • CNS prophylaxis Intrathecal C/T Cranial irradiation • Bone marrow transplantation
Management and treatment • Hydration, prevention of hyperuricemia and tumor lysis syndrome. • Antibiotics, may need the 3rd generation of cephalosporin or other strong antibiotics, even antifungal agents.
Management and treatment • Blood transfusion(component therapy) • Nutritional support • Bone marrow transplantation • Growth factor
Treatment • The primary treatment for ALL is chemotherapy. • Radiation therapy may be used in certain cases • Bone marrow transplantation is being studied in clinical trials.
Treatment : Chemotherapy Prednisone: • Used in induction and reinduction therapy and also given as intermittent pulses during continuation therapy. • toxicity : fluid retention, increased appetite, transient diabetes, acne, striae, personality changes, peptic ulcer, immunosuppression, osteoporosis, growth retardation; caution in diabetes, fungal infections, and osteonecrosis
Vincristine: • toxicity : Peripheral neuropathy manifested by constipation, ileus, ptosis, vocal cord paralysis, jaw pain, abdominal pain, loss of deep tendon reflexes; reduce dosage with severe peripheral neuropathy; bone marrow depression; local ulceration with extravasation, SIADH
Asparaginase • local rash, hives, anaphylaxis; bone marrow depression, hyperglycemia, hepatotoxicity, and bleeding may occur. Daunorubicin • Myelosuppression and thrombocytopenia; may cause cardiac arrhythmias immediately following administration and cardiomyopathy after long-term use; nausea, vomiting, stomatitis, and alopecia; extravasation may occur, resulting in severe tissue necrosis; caution with impaired hepatic, renal, or biliary function.
Methotrexate (Folex PFS) • Hematologic, renal, GI, pulmonary, and neurologic systems; discontinue if significant drop in blood counts; aspirin, NSAIDs, or low-dose steroids may be administered concomitantly with MTX (possibility of increased toxicity with NSAIDs, including salicylates, has not been tested)
Treatment Induction:(10 weeks) • Prednisolone,Vincristine,Idarubicin, Asparaginase,cyclophosphamine,cytarabine, 6-MP,TIT. Consolidation:(8 weeks) • 6-MP,MTX,TIT Reinduction:(7 weeks) • Dexamethasone, ,Vincristine,Idarubicin, Asparaginase,cyclophosphamine,cytarabine, 6-MP,TIT.
Acute Leukemia:AML versus ALL • Adults - 85% of acute leukemia is AML • Children-85% of acute leukemia is ALL • Leukemic Blast morphology • AML: cytoplasmic granules, Auer rods, more cytoplasm, 2-5 nucleoli • ALL: no cytoplasmic granules, minimal cytoplasm, 1-2 nucleoli
AML:FAB classification • French American British classification • M0-M7 based on morphology, and special cytochemical studies • Historically, distinguishing AML M0 from ALL was a major clinical problem
AMLFAB classification • M0,M1, M2: Myeloblasts with no, little or some granulocytic maturation • M3: Promyelocytic leukemia • M4: Myelomonocytic or eosinophilic • M5: Monocytic • M6: Erythroleukemia • M7: Megakaryoblastic Not all that useful except for M3 or APL
Acute Leukemia:AML vs. ALL • Cytochemistry AML ALL • Myeloperoxidase + - • Sudan black + - • Non-specific esterase + (M4,5) - • PAS + (M6) + • Acid phosphatase + (M6) +
AML Treatment:Induction Chemotherapy • Anthracycline (Idarubicin) for 3 days and Cytosine arabinoside (Ara-C) for 7 days (3+7, Younger/fit patients only) • Three to 5 weeks of pancytopenia • Supportive care red cell and platelet transfusions, prophylactic antibacterial, antifungals and antivirals
AML Treatment:Allogeneic Transplant Advantages Stem cells from HLA-matched sibling or unrelated individual allow high dose therapy and are free of leukemia Immunologic graft versus leukemia effect (GVL). Results in decreased rate of leukemic relapse
Chronic myelogenous leukemia (CML) The myeloproliferative diseases (MPDs) are clonal stem cell disorders characterised by leukocytosis, thrombocytosis, erythrocytosis, splenomegaly, and bone marrow hypercelularity They are divided into polycythemia vera (PV), essential thrombocytosis (ET), myelofibrosis and chronic myelogenous leukemia (CML)
CML results from a somatic mutation in a pluripotential lymphohematopoietic cell • CML ischaracterizedby increasedgranulocyticcellline, associated with erythroid and platelethyperplasia • The disease usually envolves into an accelerated phase that often terminates in acute phase • chronic phase 3-5 years • accelerated phase • blastic phase 3-6 months
The bcr/abl fusion protein • Uncontrolled kinase activity • Deregulated cellular proliferation • Decreased adherence of leukemia cells to the bone marrow stroma • Leukemic cells are protected from normal programmed cell death (apoptosis)
Clinical features • 30 percent of patient are asymptomatic at the time of diagnosis • Symptoms are gradual in onset: • easy fatigability, malaise, anorexia, abdominal discomfort, weight loss, excessive sweating • Less frequent symptoms: • Night sweats, heat intolerance- mimicking hyperthyroidism, gouty arthitis, symptoms of leukostasis (tinnitus, stupor), splenic infartion (left upper-quadrant and left shoulder pain), urticaria (result of histamine release) • Physical signs: • Pallor, splenomegaly, sternal pain
Laboratory features • The hemoglobin concentration is decreased • Nucleated red cells in blood film • The leukocyte count above 25000/μl (often above 100000/μl), granulocytes at all stages of development • Hypersegmentated neutrophils • The basophiles count is increased • The platelet count is normal or increased • Neutrophils alkaline phosphatase activity is low or absent (90%)
Laboratory features (2) • The marrow is hypercellular (granulocytic hyperplasia) • Reticulin fibrosis • Hyperuricemia and hyperuricosuria • Cytogenetic test- presence of the Ph chromosome • Molecular test – presence of the BCR-ABL fusion gene
Differential diagnosis • Polycythemia vera • Myelofibrosis • Essential thrombocytemia • Extreme reactive leukocytosis
Treatment • Oral chemotherapeutic agents (hydroxyurea, busulfan) • Interferon alfa • Imatinib mesylate (Glivec, Gleevec)-Inhibits activity of mutant tyrosine kinase by blocking ATP binding • Allo- SCT
Blast phase (blast crisis) of CML • Criteria of blast phase • Blasts ≥20% • extramedullary tumors • Phenotype of blasts • Mieloblasts - 50% • Limphoblasts - 30% • Megakarioblasts – 10% • Acute myelofibrosis