Download
1 / 62
820 likes | 1.97k Vues
Diagnosis and Management Of Acute Leukemia in Children and Adolescents. Grand Rounds September 20, 2010 St. Elizabeth Hospital, Lafayette, Indiana Bassem. I. Razzouk, MD, FAAP Medical Director, St. Vincent Children’s Center For Cancer & Blood Diseases. Pediatric Cancer Incidence USA.

E N D
Diagnosis and Management Of Acute Leukemia in Children and Adolescents Grand Rounds September 20, 2010 St. Elizabeth Hospital, Lafayette, Indiana Bassem. I. Razzouk, MD, FAAP Medical Director, St. Vincent Children’s Center For Cancer & Blood Diseases
BFU-E/CFU-E CFU-GM CFU-Baso CFU-Eos Hematopoiesis PLURIPOTENT STEM CELL MIXED PROGENITOR CELL COMMITTED PROGENITOR CELL RECOGNIZABLE BONE MARROW PRECURSOR CELL MATURE BLOOD CELL pronormoblast red cell myeloblast monoblast neutrophil monocyte eosinophil myeloid progenitor cell basophil CFU-Meg megakaryocyte platelet pluripotent stem cell pre-T lymphoblast T-cell pre-B lymphoblast B-cell lymphoid progenitor cell & plasma cell
myeloblast promyelocyte myelocyte metamyelocyte band neutrophil Myeloid Maturation MATURATION Adapted and modified from U Va website
Principles of leukemogenesis • A multistep process • Neoplastic cell is a hematopoietic pleuripotent cell or early myeloid cell • Dysregulation of cell growth and differentiation (associated with mutations) • Proliferation of the leukemic clone with differentiation blocked at an early stage
Classification of Leukemias Acute Chronic Myeloid origin Acute Myeloid Leukemia (AML) Chronic Myeloid Leukemia (CML) Lymphoid origin Acute Lymphoblastic Leukemia (ALL) Chronic Lymphocytic Leukemia (CLL)
Acute Leukemia • Accumulation of blasts in the marrow
Epidemiology • Childhood leukemia represents 12% of all leukemias; 60% of all acute lymphoblastic leukemias • Leukemia is the most common cancer diagnosed in children at 4.3/100.000
Epidemiology • ALL/AML = 5 • Peak incidence • ALL: 2 to 5 years • AML: 1 year, increases with age • Boys > girls • T-cell 4 times greater incidence • Infant leukemia > in girls
Significance of Acute Leukemia • A hematologic urgency/emergency • Usually fatal within weeks to months without chemotherapy • With treatment, moderate to high morbidity ( acute and long term) due to disease or treatment-related complications • Notify Peds H/O promptly if acute leukemia is suspected
Causes of Acute Leukemias • Idiopathic (most) • underlying hematologic disorders • chemicals, drugs • ionizing radiation • viruses (HTLV I) • hereditary/genetic conditions
Predisposing Factors • Genetic Syndromes • Down syndrome: 10-20 times increased incidence (600 times in megakaryoblastic type) • Bloom syndrome • Neurofibromatosis • Schwachman syndrome • Ataxia Telangiectasia • Klinefelter syndrome
Predisposing Factors • Familial aggregation • Concordance in Twins • High birth weight • Ionizing radiation • Non-ionizing radiation (?EMF) • Alcohol consumption/cigarette smoking • Breast feeding has protective effect
Clinical Manifestations • Symptoms due to: • marrow failure • tissue infiltration • leukostasis • constitutional symptoms: Fever, weight loss, night sweats, anorexia • other (DIC) • Usually short duration ( 4-8 weeks)
Clinical Presentation Very heterogenous • Pallor • Petechiae • Hepatosplenomegaly • Adenopathy • Fever • Bony pain
Infiltration of tissues/organs • Enlargement of liver, spleen, lymph nodes • Gum hypertrophy • bone pain • other organs: CNS, skin, testis, any organ
Chloromas • Granulocytic Sarcoma (myeloblastoma) • Localized mass of primitive myeloid cells that infiltrate extramedullary sites • Involvement of every organ system has been reported
Leukostasis • Accumulation of blasts in microcirculation with impaired perfusion • lungs: hypoxemia, pulmonary infiltrates • CNS: stroke • Mostly seen with WBC >> 50 x 109/L in AML and > 100 X109/L in ALL
Differential Diagnosis • Juvenile Rheumatoid Arthritis- caution to use steroids / oral methotrexate before completely ruling out leukemia • Mycobacterial infections ( TB & non-TB) • Infectious mononucleosis • Aplastic anemia • Neuroblastoma • Rhabdomyosarcoma • Hypereosinophilic syndrome
Laboratory Data • White blood cell count: variable • Hemoglobin levels: low • Platelet count: low • Serum chemical values • Uric Acid and LDH: elevated • Calcium: elevated • Chest X-ray: Mediastinal Mass; Preferable to do CXR with initial diagnosis of asthma, especially if you plan to use steroids • Coagulation screening: abnormal
WBC < 10.000 53% 10,000-49,000 30% > 50,000 17%
Newly Diagnosed Patients withLeukemia- Work-up • Establish a diagnosis Peripheral blood and bone marrow studies Morphology Immunopathology (cell markers) Cytogenetics Molecular Genetics • Risk assessment • Protocol enrollment- patients enrolled on clinical trials have better outcome • Consent Process
Bone Marrow Aspirate/Biopsy • Necessary for diagnosis: Aspirate for ALL; Aspirate/biopsy for AML • Useful for determining type • Useful for prognosis • Acute leukemias are defined by the presence of > 20% blasts (AML) or 25 % blasts (ALL) in bone marrow (% of nucleated marrow cells)
Diagnosis Morphology, cytochemistry and immunophenotype Leukemia • Acute vs. Chronic • Lymphoid vs. Myeloid
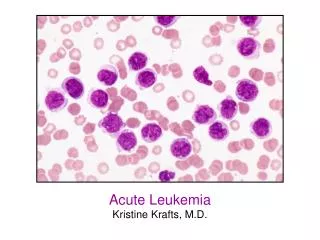
Morphology/ Cytochemistry
Key Points In ALL And AML The childhood acute leukemias are a very heterogeneous group of diseases Accurate diagnosis is important Selection of optimal therapy is pivotal
Blood Cells Immunophenotype
Immunologic Classification Lymphoid CD3, CD7, CD10, CD19, CD79 Myeloid M6/M7 CD41a, CD61, and CD42b FVIII Hemoglobin Lymphoid Vs. M0-M7
Genetics of Childhood ALL • B-lineage ALL Translocation Fusion Incidence Cure rates t(12;21) TEL-AML1 25% 90% t(1;19) E2A-PBX1 5-6% 75% t(4;11) MLL-AF4 2-5% 35% t(9;22) BCR-ABL 3-5% <30% (70 % ) with TKI’s
AML-associated chromosomalabnormalities Abnormality Fusion FAB Incidence t(8;21) AML1-ETO M2 15% inv (16) CBFβ-MYH11 M4Eo 8-12% t(15;17) PML-RARM3 8- 10% t(9;11) MLL-AF9 M4,M5 7% t(11;19) MLL-ELL M4, M5 1% t(1;22) Unknown M7 1%
PROGNOSTIC FACTORS survival Tx DISEASE Heterogeneity Intensity Specificity
Prognostic Factors - ALL • Initial white blood cell count • Age at diagnosis • Immunophenotype • Genetic Features • Extramedullary involvement ( CNS, testis) Response to therapy
ALL- Risk Groups St. Jude Estimated COG Low 40% Standard Standard 50% High High 10% Very High
Prognostic Factors- AML • Favorable • Age < 1 year of age • Genetics: t(15;17), inv16, t(8;21) and t(1;22) • Down syndrome • Intermediate • Genetics: normal karyotype, other 11q23 • Residual disease after induction • High-risk • Cytogenetics: -7, -5, t(6;9), complex karyotype • AML arising from MDS • Persistent disease after induction