Download

1 / 45
570 likes | 947 Vues
Acute Leukemia. L. Larratt. Leukemia. Acute myeloid lymphoid Chronic myeloid lymphoid. “White Blood” cancer of the bone marrow cells. Leukemia. Proliferation of a clone of hematopoietic cells poorly responsive to normal regulatory mechanisms failure of maturation

E N D
Acute Leukemia L. Larratt
Leukemia • Acute myeloid lymphoid • Chronic myeloid lymphoid • “White Blood” • cancer of the bone marrow cells
Leukemia • Proliferation of a clone of hematopoietic cells • poorly responsive to normal regulatory mechanisms • failure of maturation • may inhibit growth of normal cells
Leukemia • 3 - 4 / 100,000 US • AML 80% adults 30% > 60 y • ALL 80% pediatrics peak 3 - 4 y • ALL most common pediatric malignancy
Etiology of Leukemia • Radiation • Chemicals • alkylating agents, arsenic,benzene, ?phenylbutazone,?chloramphenicol • Hereditary • Down’s1/95, Bloom’s 1/8, Fanconi’s anemia, ataxia telangiectasia, congenital agammaglobulinemia, identical twin ALL 25%
Etiology cont. • Hematological Diseases • Myelodysplastic syndromes • Myeloproliferative disorders • Multiple Myeloma • Paroxysmal Nocturnal Hemoglobinuria • Viruses HTLVI, Feline Leukemia virus • Oncogenes t8:14 c myc Burkitt’s • Idiopathic most common
Clinical presentation • Nonspecific i.e. fatigue , wt loss • Bleeding • Infections • CNS disease • bone pain • gout • testicular mass • Leukemia cutis
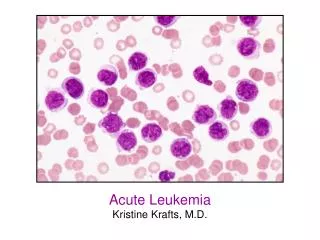
Laboratory Assessment • Peripheral blood film • Bone marrow • Coagulation Profile • Biochemistry • liver and renal function • uric acid • LDH • Calcium • Microbiology
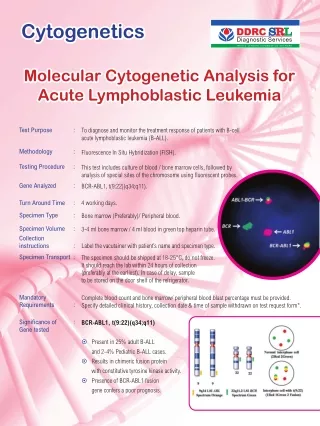
Bone Marrow Assessment • Morphology need > 20% blasts • Surface Markers • Histochemistry • Electron Microscopy • Cytogenetics • Molecular Markers eg flt3, ckit etc • Immunoglobulin & T cell Receptor Rearrangement
Facts • M3 Acute Promyelocytic Leukemia • associated with DIC • Treated with retinoic acid in combination with chemotherapy with favorable results • Data using arsenic in initial disease and relapse emerging • M5 Acute Monocytic Leukemia • associated with gingival hyperplasia • AML with risk of CNS disease
Markers • AML : range of myeloid markers • ALL : tdt +, CALLA + for common ALL Ag in children
Treatment • Supportive management • transfusions • nutrition • allopurinol / fluids and electrolytes • management of fevers • psychosocial support
Specific Therapy • Induction • Consolidation • Maintenance • CNS treatment • Bone Marrow Transplant
AML • Backbone of AraC and an anthracycline • No maintenance therapy except acute promyelocytic leukemia (APL) • Treatment usually 3 – 6 months • Pt are considered for a stem cell transplant if younger than 65 for intermeidate and high risk leukemia • SCT for AML with favorable characteristics in 2nd remission
AML • Generally • CR high 60 - 70 • DFS low 20 - 30 % • BUT Results very dependent on leukemia characteristics with wide range of DFS • <10% secondary leukemia with complex cyto • 65% with favorable cyto 8:21 or inv 16 • 90% with apl • Dependent on pt ability to have treatment as well (comorbidity)
ALL • ALL : Induction therapy includes steroids,vincristine, anthracycline & asparaginase • CNS management essential as often involved at presentation or as a sanctuary site • Maintenance therapy with full therapy up to 3 years • CR 80 - 90%, DFS 40 - 50% in adults children often superior results • Older pt often have Ph chrom + disease
Contrast • ALL • No rods • children • Long treatment (3y)) • CNS disease • Testes sanctuary site • 40 - 50% cures higher in children • AML • Auer rods • adults • shorter treatment • low CNS risk • No sanctuary sites • 20 - 30% DFS
Case 3 • A 63 year old male presents with fever, fatigue, general malaise. He is bleeding from his nose and oral mucosa. He has multiple bruises and petechiae. He complains of a sore throat and is experiencing more anginal symptoms. • His temp is 39 HR 110 BP 95/60 • Diaphoretic, No LN or splenomegaly • Gingival hyperplasia
Case 3 LAB • Hb 65 MCV 90 • WBC 110,000 95% Blasts Auer rods • Platelets 10,000 • PT 1.4 PTT 48 • Fibrinogen 1.0 Dimers + • Uric Acid 800 LDH 3X normal • Creatinine 150 Potassium 2.8 • Liver tests Normal • EKG non specific changes
Case 3 : AML • Priorities • ABC • Early septic shock • Febrile Neutropenia • Transfusion • Packed cells, platelets, DIC management • Cardiac Status
AML Management • Supportive Care • Bowel care • Mouth care • Diet • Uric acid • Potassium • Transfusion support • Psychological support / social services
AML Management • Leukostasis • Tumor Lysis • DIC • Specific Therapy • Induction • Consolidation • BMT
MYELODYSPLASTIC SYNDROMES • Acquired abnormality of bone marrow characterized by progressive bone marrow failure with quantitative and qualitative abnormalities of all three cell lines • Cellular marrow • Ineffective hematopoiesis • Cytopenias
FAB Classification • Refractory anemia • Refractory anemia with ring sideroblasts • Refractory anemia with excess blasts (RAEB) ( 5 – 20 % ) • RAEB in transformation ( blasts 20 – 30 %) This is eliminated now as now dx AML • Chronic myelomonocytic Leukemia
Etiology • 1o often older patients • 20 post cytotoxic drugs • Incidence up to 5 % with some chemotherapy regimens • Varies re alkylators vs topomerases
MDS • Cytopenic presentations • Anemia • Neutropenia • Thrombocytopenia • Laboratory • Early macrocytosis then progressive cytopenias
Management • Supportive : transfusions, vitamin therapy, iron chelation • Growth Factors epo, g csf • Revlimid 5q- disease • Differentiating agents like azacitidine • Immunosuppressive therapy ATG/Cyclosporin • Chemotherapy (mainly for high risk MDS) • Stem cell Transplant
Mortality of MDS • Infection • Bleeding • Transformation to Acute Myeloid Leukemia • More difficult to manage than de novo leukemia • Lower response rates • Incurable unless BMT
Prognosis • Low Risk • Years with support • Live long enough to have iron overload from transfusions • High Risk • Months unless sct or successful treatment with agents like azacytidine Generally the secondary mds behave aggressively and treatment again limited by age and comorbidity