Download
1 / 36
360 likes | 498 Vues
Bladder Carcinoma. DR. Gehan Mohamed. Bladder Carcinoma. Definition: malignant tumor arising from the epithelial lining of the urinary bladder.

E N D
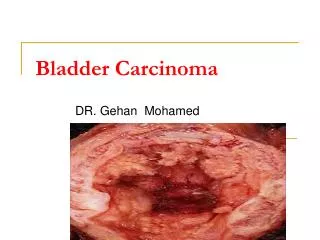
Bladder Carcinoma DR. Gehan Mohamed
Bladder Carcinoma • Definition: malignant tumor arising from the epithelial lining of the urinary bladder. • (N.B normal epithelial lining of urinary bladder is transitional epithelium but it can change to squamous epithelium or columnar type under the effect of continuous irritation by inflammation, or stone formation)
transitional epithelium (urothelium) lining the normal urinary Bladder.
Epidemiology of Bladder Carcinoma • Caucasians ~ 2x > African Americans > Hispanics & Asians • M:F = 3:1 • age 40 : 60 years.
Risk Factors for Bladder Cancer 1- Genetics (eg, Retinoblastoma gene mutation which is tumor suppresor gene present on chromosome 13 undergo hereditary or aquired mutation so lost its function ). 2- Bladder birth defects eg. persistent urachus increase risk for adenocarcinoma. Urachus is a connection between belly button(umblicus) and bladder. Normally disappears before birth. If part of the connection remains, it could become cancerous. Cancers that start in the urachus are usually made up of malignant glandular cells and are called adenocarcinomas. 3-Pelvic radiation exposure
Risk Factors for Bladder Cancer 4-Cigarette smoking (2-4x higher relative risk) Some carcinogens in tobacco smoke are absorbed from lungs and get into blood. From there, they are filtered by kidneys and concentrated in urine. These chemicals in the urine damage the urothelial cells(transitional epithelium) that line the inside of the bladder increase Carcinoma risk. 5-Cyclophosphamide A highly toxic, immunosuppressive, antineoplastic drug 9 fold increase risk 6- Arsenic 7- Occupational Exposuresto chemicals: Polycyclic aromatic hydrocarbons, benzidine, benzene, exhaust from combustion gases. Al+3 workers; dry cleaners; manufacturers of preservatives, dye, rubber, & leather; pesticide applicators; painters; truck drivers; printers; machinists. (N.B Low fluid intake increase exposure to any chemical carcinogens via decreased bladder emptying.)
Risk Factors for Bladder Cancer 8- Infections • Schistosomahaematobium (North Africa) Increase risk for squamous & transitional cell Carcinoma. • Schistosomahaematobium formation of carcinogenic substance N-nitroso compounds increased risk for both squamous and transitional cell Carcinoma. 9- bladder stones cause chronic irritation to the mucosa so increase risk for squamous cell metaplasia Cancer.
Microscopic types of Bladder Canrcinoma • 1- Transitional cell carcinoma (> 95%) • Flat – Do not grow toward the hollow part of the bladder. • Papillary (70%) – Grow toward the hollow part of the bladder. • 2- Squamous cell (keratinizing) carcinoma (1-3%) on top of squamous metaplasia. • 3- Adenocarcinoma (1-2%) . • 4- Small cell carcinoma (< 1%) • 5- spindle (sarcomatoid ) carcinoma • 6-Mixed-histology (predominantly transitional cell with other types).
Squamous cell carcinoma showing keratinized nests of squamous epithelium
Adenocarcinoma : tumor cells form glands with malignant criteria , and deeply infiltrating Cytokeratin +
Diagnosis of bladder cancer • 1- clinical picture • 2- investigations to confirm diagnosis ,determine the histologic type, grade, and detect its extent. • 3- immunohistochemistry using cytokeratin which is positive with malignant tumor arising from epithelium(carcinoma)
Clinical Manifestations of Bladder CA 1- Hematuria (80-90%) – Generally painless and may be gross or microscopic hematuria. (it must be differentiated from other causes of hematuria as cystitis,prostaticleison) 2-Pain : often reflects tumor location • Lower abdominal pain – Bladder mass • Rectal discomfort & perineal pain – Invasion of prostate or pelvis. • Flank pain - Obstruction of ureters 3- Other urinary Symptoms: • Frequency, urgency, nocturia due to irritation of the mucosa or due to decrease bladder capacity.
investigations for Bladder Cancer • Investigations are recommended forPatients with hematuria, especially if > 40 years • Urinary Cytology to detect any desquamated malignant cells. • Cystoscopy, regardless of cytology results (main stay of dx) • Transurethral resection of all visible tumors to determine histology & depth of invasion • Biopsies of erythematous areas to assess for carcinoma in situ (CIS)i.e malignant cells still present in its place and not invade basement membrane.
investigations for Bladder Cancer • Imaging • cystoscopy • Ultrasonography • CT, or MRI - Can help determine extent of tumor spread (eg, into perivsesical fat, prostate or vagina, LNs) • CT chest / abdomen, MRI, radionuclide imaging of skeleton to assess for distant mets
Grading of transitional cell carcinoma( i.e evaluating degree of similarity of the malignant cells to its normal counterpart) • 1- low grade : if tumor cells are less pleomorphic,slightly similar to the cell of origin ,few mitosis, so have better prognosis. • 2- high grade : worse prognosis because it have aggressive behavior, more infiltrative As the cells highly pleomorphic, have more mitosis.
TNM staging for bladder carcinoma • T is tumor • N express lymph node affection by the tumor so : N0 no affection to lymph nodes. N+ the lymph nodes are infiltrated by the tumor • M express distant metastasis so : M0 no distant metastasis M+ there is distant metastasis.
Pathologic evaluation of bladder carcinoma tumor (PT) • In PT 0,abnormalcells are found in tissue lining the inside of the bladder. Stage 0 is divided into stage 0a and stage 0is, depending on the type of the tumor: - PT 0a is also called papillary carcinoma, which may look like tiny mushrooms growing from the lining of the bladder. - PT 0is is also called carcinoma in situ, which is a flat tumoron the tissue lining the inside of the bladder. • In PT I, cancer has formed and spread to the layer of tissue under the inner lining epithelium of the bladder . • In PT II, cancer has spread to either the inner half or outer half of the muscle wall of the bladder.
Staging of bladder carcinoma • In PT III, cancer has spread from the bladder to the fatty layer of tissue surrounding it and may have spread to the reproductive organs (prostate, seminal vesicles, uterus, or vagina). • In PT IV, cancer has spread from the bladder to the wall of the abdomen or pelvis. Cancer may have spread to one or more lymph nodes or to other parts of the body.
Bladder cancer: Stage and Prognosis TNM stagging Stage 0 Ta/Tis NoMo Stage I T1 NoMo Stage II T2a-b NoMo Stage III T3a-4a NoMo Stage IV T4b NoMo any T N+Mo any T M+
Complications of urinary bladder carcinoma • 1- bleeding • 2-Obstruction specially if the tumor grow near the urethral opening of the bladder lead to Bilateral Obstructive Uropathy in the form of hydroureter,hydronephrosis • 4- Kidney Stones secondary to the obstruction and infection. • 5- enterovesicular fistula is an abnormal channel that connects the interior of the urinary bladder with another structure within the abdomen. This can be found in cases of squamous cell carcinoma. This condition can present as gas or air in the urine. Repeated urinary tract infections may possibly occur if the urinary bladder becomes connected with the intestine
6- spread of the malignant tumor either by : a- direct spread to surrounding structures b- hematogenous spread to distant organs. c- lymphatic spread.
Treatment & Prognosis of Superficial Bladder Carcinoma • Requires at least complete endoscopic resection +/- intravesical therapy using Bacillus Calmette-Guérin (BCG) vaccine which act through stimulation of the immune system in such a way that the immune system begins to target and destroy any remaining cancer cells.
Treatment of Muscle-Invasive Bladder Carcinoma • Generally radical cystectomy & pelvic lymphadenectomy • Removal of bladder & pelvic LNs with creation of a conduit or reservoir for urinary flow. • + Removal of prostate, seminal vesicles, & proximal urethra in males. Generally impotence. • + Removal of urethra, uterus, fallopian tubes, ovaries, anterior vaginal wall, & surrounding fascia in females.
Treatment of Muscle-Invasive Bladder Carcinoma • Concomitant Chemotherapy & Radiation • For those with a solitary early-stage lesion and no hydronephrosis • Generally use Cisplatin