Download
1 / 40
400 likes | 593 Vues
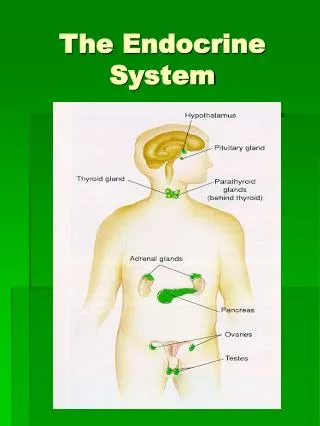
Diseases of the endocrine system. Review hormones. Anterior pituitary GH TSH ACTH FSH LH Prolactin MSH Posterior pituitary Vasopressin (ADH) Oxytocin Thyroid T3, T4 Parathyroid PTH Adrenal cortex Aldosterone Cortisone Androgens, estrogens, progestins. Review.

E N D
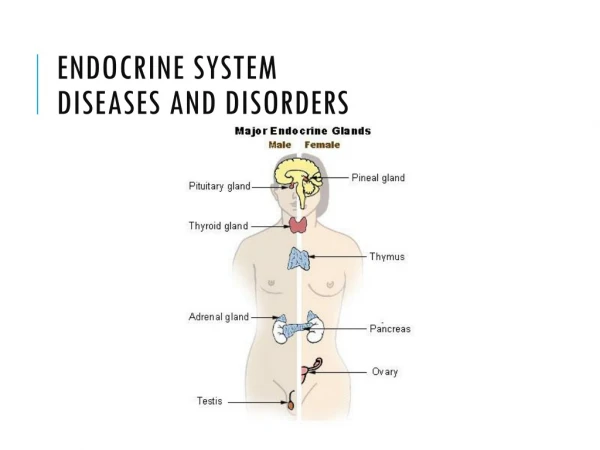
Review hormones • Anterior pituitary • GH • TSH • ACTH • FSH • LH • Prolactin • MSH • Posterior pituitary • Vasopressin (ADH) • Oxytocin • Thyroid • T3, T4 • Parathyroid • PTH • Adrenal cortex • Aldosterone • Cortisone • Androgens, estrogens, progestins
Review • Adrenal Medulla • Catecholamines: epinephrine, norepinephrine • Pancreas • Insulin • Glucagon • Ovaries • Estrogens • Progesterone • Testes • Testosterone • Thymus • Thymosin – promotes development of immune cells – gone in adulthood due to atrophy • Pineal gland • melatonin
Hyperpituitarism • Mainly increase in hGH • Chronic and progessive
Gigantism • Increase hGH in childhood • S/S • Proportional increase in size because epiphyseal closure has not occurred yet • Abnormal and accelerated growth • Often caused by an adenoma (cancer) • Dx: CT and blood levels of hGH • Tx: radiation or surgery usually
Acromegaly • Increase hGH in adulthood • S/S • Overgrowth of face, hands, and feet • Overgrowth of soft tissues • Dx and Tx same as gigantism
Dwarfism • Hypopituitarism in childhood • Underdevelopment of the body often caused by lack of hGH • Many causes • Tx: hormone replacement when needed
Diabetes Insipidus • Not same as diabetes you hear about from the media • Disturbance of water metabolism • S/S • Polyuria, polydipsia, signs of dehydration, such as dry mucous membranes, hypotension, dizziness, constipation, and poor skin turgor • Tx: replacement • DDAVP (desmopressin acetate)
Hyperthyroid • High T3, T4 production • Low TSH levels • S/S • Tachycardia, nervousness, excitability, insomnia, weight loss, tremor, loss of hair. • In advanced, exophthalmos (outward protusion of eyes) • Sudden exacerbation can indicate life-threatening condition, such as thyrotoxicosis (thyroid storm)
Hyperthyroidism • Dx: TSH, T3, and T4 levels. If concerns, thyroid scan • Tx: • B-blocker for tachycardia • PTU or Tapazole to stop thyroid production • Radioactive Iodine for curative measures • Will “kill” the thyroid • Will need thyroid replacement afterwards for life • NEVER performed if pregnant because will destroy mother’s and child’s thyroid
Hyperthyroidism • Graves disease • Form of hyperthyroidism • Body produces antibodies against thyroid, which connect and mimic TSH causing large increase. • Thyroid will eventually “burn out” over time causing hypothyroidism • Can form a goiter
Hypothyroid • Low T3, T4 • High TSH levels • S/S: • Dry skin, fatigue, weakness, weight gain, loss of hair, constipation, intolerance to cold • Dx: TSH levels • Tx: Levothyroxine (synthroid) for life • Severe cases cause Myxedema
Hypothyroidism • Cretinism • Hypothyroidism in infancy • S/S • Mental and growth retardation, stocky stature with protruding abdomen, lack of muscle tone contributing to inability to stand or walk, slow to smile in infancy • Part of Metabolic screening required at birth
Thyroid cancer • Hard, painless lump or nodule on thyroid. • Some exhibit dysphagia or hoarseness
Hyperparathyroidism • Causes high blood calcium • S/S: • Muscle weakness and paralysis, heart conduction problems, kidney stones, breakdown of bones causing increase risk for fractures • Dx: • High PTH, calcium, chloride, and alkaline phosphatase. • Low serum phosphorus. • Tx: depends on cause
Hypoparathyroidism • Causes low blood calcium • S/S: • Hypocalcemia, overstimulation of skeletal muscle, numbness, tingling, muscle spasms • Dx: • Low serum calcium • High serum phosphate • Tx: depends on cause. Calcium and Vit D supplementation
Cushing syndrome • High cortisol levels • S/S: • Fatigue, weakness, changes in body appearance, weight gain. • Fat deposits on scapular area (buffalo hump) and abdomen. Moon face. Acne • Hypertension, edema, hyperlipidemia, osteoporosis, atherosclerosis, diabetes mellitus • Increase risk of infection due to suppression of immune response • Excessive hair growth, amenorrhea, impotence
Addison Disease • Low to none aldosterone and cortisol • Several symptoms including hyperkalemia • Tx: replacement of hormones
Diabetes Mellitus • Either inadequate production of insulin by the pancreas or faulty utilization of insulin by the cells. • S/S: • Polydipsia, polyuria, fatigue, weight loss, hyperglycemia • Several forms including • Insulin dependent diabetes mellitus (IDDM) (Type 1) • Non-insulin dependent diabetes mellitus (NIDDM) (Type 2) • Gestational diabetes
Background • Insulin is secreted by the pancreas, connects to different cells on receptors causing glucose to go from the blood into the cell. As a result, blood glucose levels decrease. • If enough insulin is not released, then glucose will remain elevated in the blood • If the receptors are not working well, the insulin will not work causing the blood glucose levels to remain high
Background • If glucose cannot get into the cells, then another source must be used, which is fat and protein, resulting in production of waste products called ketones. Ketones increase the acidity of the blood (lower pH). They also produce a fruity odor on the breath.
Chronic consequences • Atherosclerosis resulting in MI and CVA • Retinopathy resulting in blindness • Neuropathy • Renal failure • Delayed healing • More prone to infection • PVD resulting in foot ulcers
IDDM (type 1) • Usually in childhood • Often antibodies destroy B-cells of pancreas resulting in no insulin production • Tx: insulin replacement
NIDDM (type 2) • Usually in adulthood but seen now in obese children • Patient often overweight or a family Hx • Produces enough insulin but receptors are not responding appropriately • Tx: oral medications first, then insulin
Dx • Fasting blood sugar over 126 on two separate occasions results in a diagnosis • Fasting blood sugar between 101-125 is considered glucose intolerance • A1C • Blood test measures how sugars have been running for past 3 months • Depending on source, A1C should be <7.0 or <6.5 • A non-diabetic will have an A1C <6.0
Screening at exams • Yearly eye exams • #1 cause of blindness • Foot exams • #1 cause of amputations • Cholesterol • Blood pressure • Smoking • Micro-protein in urine once/year • #1 cause of kidney failure
Oral Treatment • Sulfonylureas • Glipizide, glyburide, amaryl • Increases insulin release • Side effect of hypoglycemia • Metformin • Increases receptor response • Side effect of GI disturbance • Thiazolidinediones (TZD) • Actos, Avandia • Increases number of receptors • Side effect of edema – not to be used in CHF
Insulin • Several different forms including long-acting and short-acting • Required to be injected • Lantus most common long-acting • Lasts 24 hours • Won’t cause hypoglycemia in most cases
Other treatment • Diabetic education • Nutritional education • Education on how to use meters • Regular checking sugars • Weight loss for type 2
Gestational diabetes • Diabetes occurring during pregnancy • Important to monitor closely • Make cause large babies • Usually resolves after delivery but not always • Some oral medications may be used but not all • Usually requires insulin
Hypoglycemia • S/S • Sweating, nervousness, weakness, hunger, dizziness, trembling, headache, palpitations, confusion, abnormal behavior, coma • Brain’s fuel source is glucose – cannot use fat or glycogen, so low sugar causes CNS symptoms • Most commonly drug-induced • Insulin, sulfonylureas, alcohol, excessive exercise, ect… • Tx: increase glucose and correct underlying cause • If idiopathic, then diet modification. No medications for long-term Tx