Download
1 / 19
220 likes | 323 Vues
Explore the classification, diagnosis, and treatment strategies for bile duct injury during laparoscopic cholecystectomy. Learn about the potential complications, presentation, and surgical intervention options.

E N D
Dr. Hung KaWai Ray Team 1 Hepatobiliary and Pancreatic Surgery Prince of Wales Hospital Classification and management of bile duct injury
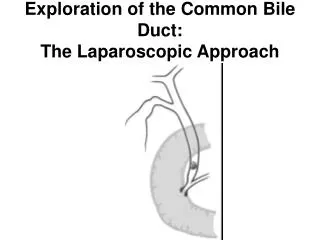
Laparoscopic cholecystectomy • Standard treatment of symptomatic gallstone disease • > 750, 000 were performed annually in the United States • Less pain, fewer wound complication, quicker recovery • The only potential disadvantage is a higher incidence of major bile duct injury [1], 0.3% open vs 0.6% laparoscopic Introduction
Bile duct injury is a very serious complication that lead to mortality, significant morbidity and impaired quality of life • Causes: • Iatrogenic • Cholecysectomy (80-85%) [2] • Gastrectomy • Pancreatectomy • ERCP • Trauma • Duodenal ulcer Introduction
Intraoperative • Direct observation of a divided duct • Bile in the operative field • Abnormal intra-operative cholangiography • Postoperative • Bile leak • Bile in the drain • Biloma, biliary fistula, or bile ascites • Bile peritonitis in severe cases • Biliary obstruction • Obstructive jaundice • Cholangitis Presentation
Bismuth • Strasberg et al. • Stewart et al. • McMahon et al. • AMA • Neuhaus et al. • Csendes et al. • Hanover • Lau and Lai • Siewert et al. • Cannon et al. • Kapoor Sandha et al. • EAES Classification
Depend on the timing of recognition of the injury • Intraoperative vs postoperative recognition Management
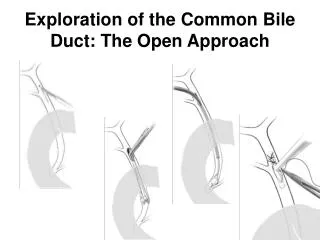
Account for 25%–32.4% [3] • First consult an experienced hepatobiliary surgeon • Convert to laparotomy with cholangiography • Define the nature of the injury • If expertise a/v • Immediate repair can minimize the morbidity • Higher successful rate, fewer morbidty and mortality [4] • If expertise not a/v • Injudicious attempts at exploration may cause further biliary and vascular injury • Subhepatic drain to prevent collection • External biliary drainage • Refer to a specialized hepatobiliary unit Intraoperative recognition
Aim of management • Control sepsis and limit inflammation • Delineate the biliary anatomy and associated vascular injury • Re-establish the biliary enteric continuity Postoperative recognition
Fluid resuscitation • Broad spectrum antibiotic • Investigation • USG / CT to asses collection +/- drainage Control sepsis
Cholangiography • ERCP • PTC • MRCP Delineate the biliary anatomy
CTA / MRA • Incidence is around 16.7%-47%[6] • Most commonly involving the right hepatic artery • Does not usually lead to early significant complications • Impact on bile duct injury [7] • Associated with increased intraoperative bleeding during repair • Difficult reconstruction • Higher incidence of anastomotic stricture due to bile duct ischamemia • Delayed repair if VBI is present Associated vascular injury
According to the type of injury Surgery vs endoscopic treatment Re-establish the biliary enteric continuity
Stricture • Balloon dilatation and biliary stenting • Hepaticojejunostomy has higher successful rate • Secondary biliary cirrhosis • Liver transplantation Treatment of Complication
[1] Acute bile duct injury. The need for a high repair. Surg Endosc 2003;17: 1351-1355 [2] Bile duct injuries during laparoscopic cholecystectomy: primary and long term results from a single institution. Surg Endosc 2007; 21: 1069-1073 [3] Stewart L, Way LW. Bile duct injuries during laparoscopic cholecystectomy.Factors that influence the results of treatment. Arch. Surg. 1995; 130: 1123–8. [4] Surgical management of bile duct injuries sustained during laparoscopic cholecystectomy: perioperative results in 200 patients. Ann. Surg 2005;241:786-90 Reference
[5] Laparoscopic bile duct injuries: timing of surgical repair does not influence success rate. A multivariate analysis of factors influencing surgical outcomes, HBP2009, 11, 516-522 [6] Management and outcome of patinets with combined bile duct and hepatic arterial injuries after laparoscopic cholecystectomy. Surgery 2004; 135: 613-8 [7] Management of bile duct injury after laparoscopic cholecystectomy: a review, ANZ J Surg 80 (2010) 75-81 Reference