Download
1 / 18
270 likes | 820 Vues
Admission &discharge of patient from hospital. Dr. Kareema Ahmed Hussein 2017 -2018. Introduction: Admission the patient to the hospital is whether scheduled or follows emergency . The goals of admission of patient. To assess the clinical status of patient.

E N D
Admission &discharge of patient from hospital Dr. Kareema Ahmed Hussein 2017 -2018
Introduction: Admission the patient to the hospital is whether scheduled or follows emergency. The goals of admission of patient. • To assess the clinical status of patient. • Make him as comfortable as possible in his new environment. • Complete the treatment that he/ she need to become well being.
Admission process: It is the process of dealing with a patient that include all steps from receiving the patient who admitted to the hospital till discharging him, which include all the measure carried out by hospital workers in order to help pt. a just to there new environment.
Types of admission: The pt's. entering the hospital through the: I Emergency unit: In which the patient is transported directly to a nursing division, while to family members provide pertinent information for hospital records . 2-Dr's recommendation. 3-Referred from private clinical.
Transportation of patient to the nursing department: I -Formal admission to the patient to the nursing department this allow nursing staff to prepare a room and obtain necessary equipment for arrival 2-Patient arrival to the ward: a- walking B-wheel chair. c-Stretcher.
3-Welcom bythe staff. 4-The nurse complete number of procedure including: a-Orientation of client to the room and unit. b-Collection of nursing history and physical assessment. c-Collection of specimen.
Preliminary admission procedures: 1-Obtain n the basic information from the patient or from his or her relatives which include: a-Full legal name b-Age. c-Birth date. d-Sex. c-Address. d-Religion
e-Occupation. f-Date of admission. g-Reason of admission. h-And admitting physician. The information is placed on an admission sheet and accompanies the patient to the assigned unit
2-The patient is assigned permanent hospital identification number admitted, the number is used to identify the patient's record during hospitalization. .
Techniques that are• use by the nurse when admitting the patient: I -Check the patient's identification band to be sure of his name. 2-Introduce yourself to the patient. 4-Help the patient to undress and assist him into a comfortable position in bed. 5-Provide for privacy.
6-Explain agency routine, such as meal times, visiting hours…..Etc. 7-Place file signal device and other equipment for the patient to use. 8-0btain the patient vital signs 9-Obtain the laboratory tests.
Information that record by the nurse when the patient admitted the hospital. Information about the patient includes, his name, address, age, date of birth, religion, sex, marital status, occupation or school, telephone number, nearest relative for emergency. • Doctor recommending admission. • Provisional diagnosis. • Check vital signs (temperature, pulse, respiration and pressure). • Measure weight and recorded. • Obtained the specimen of urine, tested and charted. • All valuables and money take home by relatives. • History of disease recorded by doctors. And record the doctors order and reason for admission .
Observation made by Nurse General reaction of patient e.g. anxiety. • Cleanliness of clothes, skin, hair, mouth. • Abnormalities of skin and other structure. • Complaints of patient e.g. pain, breath lessens. • Last passing of urine, stool, menstruation. • Medication brought with patient.
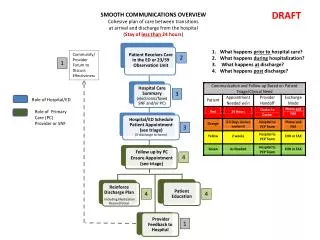
Discharge the patient from the hospital Set the decisions and activities involved in providing continuity and coordination of nursing care when a patient is discharge from health care agency. Preparation of patient at day of discharge 1-Let patient and family ask questions related to home and health care. 2-check physicians discharge order for change in treatment and instructions. 3-Determine whether the patient or family has arranged for transport at home. 4-Offer assistance as patient dresses and packs all personal belongings. 5-Provide client with prescriptions or medication ordered by physician. 6-Arrange for patient or family to visit agency -s business office for payment of bill. 7-Obtain wheel chair for patient riable to ambulate.
9-Document discharge on discharge summery form. 10-Document status of health problems at discharge. 11-From time of admission assess patient s health care needs for discharge. 12-Assess pt. and family needs for health teaching related to home therapies. 13-Assess with pt. and family environment factors within home that might interfere with self -care. 14-Collaborate with physician and other discipline. 15-Consult other health team members about needs after discharge.
Risk factors for patient discharge from the hospital • Lack of knowledge of treatment plan • Newly diagnosed chronic disease • Major surgery and radical surgery • Social isolation • Emotion or mental instability • Complex home care regime • Lack of financial recourses • Terminal illness
Discharge from hospital: • Discharge planning aims' to teach the patient and his family about his illness and its effect on his life-style. • Provide the patient instruction for home care about the diet and the activity of patient. • Arrangement made for suitable transport. • Give written instruction regarding treatment. • Follow up care if necessary, like made dressing if the patient had operation
After discharge of the patient: • Sends linen and blankets to laundry. • Sends mattress and pillow to autoclaved. • Wash the bed and table bedside. • Locker scrubbed out.