Measles in EMR
390 likes | 843 Vues
Measles in EMR. 7 th Annual Meeting of Partners for Measles Advocacy Washington, 2007. Outline. Regional progress in measles elimination Key constraints Indicators to monitor measles elimination in EMR . Strategy for Measles Mortality Reduction and Elimination in EMRO .

Measles in EMR
E N D
Presentation Transcript
Measles in EMR 7th Annual Meeting of Partners for Measles AdvocacyWashington, 2007
Outline • Regional progress in measles elimination • Key constraints • Indicators to monitor measles elimination in EMR
Strategy for Measles Mortality Reduction and Elimination in EMRO • Routine infant immunization • > 90% coverage MCV1 in all districts • Catch-up vaccination • susceptible cohorts • Second dose of measles vaccine either through a 2 dose schedule or follow-up SIAs • > 90% coverage in all districts • Case-based surveillance • Optimized case management
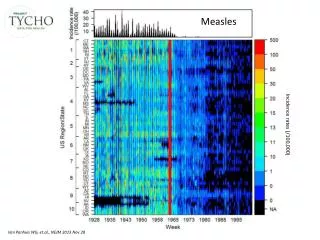
Trends in Measles Case Counts and MCV1 Coverage in EMR, 1995-2006* * Preliminary, 2006
Geographic Distribution of Children not Receiving MCV1 in EMRO, 2005 (n=2.8 million)
Supplemental Immunization ActivitiesMeasles Campaigns in EMRO through 2005 Palestine Bahrain Preschool and school age (15) School age (5) Ongoing (2)
Measles Campaign Coverage in South Sudan Status by County (Jan 28, 2007) Renk Fashoda Ruweng Tonga Aweil North Sobat Rubkoana Aweil East Mayom Twic Old Fangak Atar Aweil West Latjor Raja Guit Nyirol Gogrial Aweil South Koch Ayod Waat Leer Wuror Diror Tonj Panyijar Wau Akobo North Bor Rumbek-Cueibet Pochalla Pibor Completed Ongoing Micro plans ready Not yet micro-planned Yirol South Bor Awerial Tambura 103.4% Terekeka 101.3% Maridi 87.3% Maruko Payam missed out Kapoeta 64.2% Mundri Yambio Ezo 105.4% Juba 74.2% Budi 91.1% Torit Yei Magwi Kajo Keji
Measles Vaccine Doses Administered in Catch-up Campaigns, 1999-2006 EMRO
Reduction in Measles Mortality in EMR, 1999-2005 50% mortality reduction target
Planned Supplemental Measles Immunization; 2007-08 . Catch-up campaigns Follow-up campaigns High-risk/mop-up campaigns
Recommended SIAs in EMR that are not Planned; 2007-08 . Catch-up campaigns Follow-up campaigns High-risk/mop-up campaigns
Pakistan Catch-up Campaign • Phase 1 • Mar 2007 • 1 district in 4 provinces (2.6M target) • Phase 2 • Jul 2007 • parts of NWFP, Baluchistan, Fana, AJK (8.2M) • Phase 3 • Aug 2007 • Finish NWFP, Bal, AJK (5.3M) • Phase 4 • Nov 2007 (13.6M) • Sindh • Phase 5 • 1st Qtr ’08 (34.0M) • Punjab
Second Dose of Measles Immunization in EMRO, 2005 Palestine • 19 countries with 2 dose schedule • 12 at 12 –24 mos • 7 at 4-6 yrs • 16 use MMR • 1 countries with periodic SIAs • 2 countries with periodic SIAs and 2 dose schedule • 2 countries with no second opportunity Bahrain Routine second dose 1 dose + SIAs 2 doses + SIAs 1 dose schedule
Measles Surveillance in EMRO Palestine Bahrain Case based (17) Case-based, needs to be improved (3) Aggregate data (2)
Status of Measles Reporting in EMRO, Jan-Dec, 2006* * Provisional data, reporting not complete
Monthly Bulletin • Case counts by country and case classification • Key indicators • Mapping through EPIINFO • Website • Monitoring of susceptibility profiles Feedback of Surveillance and Coverage Data
Outline • Regional progress in measles elimination • Key constraints • Indicators to monitor measles elimination in EMR
Lack of national support for elimination • Competing priorities • Insecurity • Resource mobilization for non-GAVI countries • Egypt, Morocco, Syria • Failure of keep-up strategies • Limited use of surveillance data Key Constraints in Regional Elimination
Catch-up campaigns 12-18 yrs6-13 yrs Measles Case Counts and Vaccination Coverage, 1988-2005, Saudi Arabia Coverage
Age Distribution of Measles Cases in Saudi Arabia, Jan-Dec 2006 < 1 yr 1 to 4 yrs 5 to 9 yrs 10 to 14 yrs 15-20 yrs > 20 yrs n=697 5% vaccinated
Syria (n=462) 48% vaccinated Egypt n=998 96% vaccinated Qatar (n=108) 54% vaccinated Lebanon (n=843) 20% vaccinated Age Distribution and Vaccination Status of Measles Cases in Selected EMR Countries, Jan-Dec 2006 < 1 yr 1 to 4 yrs 5 to 9 yrs 10 to 14 yrs 15-20 yrs > 20 yrs
Outline • Regional progress in measles elimination • Key constraints • Indicatorsto monitor measles elimination
Indicators for Measles Elimination Recommendations from EMR-TAG, 2006 • Completeness of reporting • Indicator: > 80% of districts reporting on a monthly basis • Sensitivity of reporting system • Indicator: At least 2 suspect cases (excluding lab and epi-confirmed measles and rubella) per 100,000 population at the national level. • Adequacy of laboratory testing • Indicator: > 80% of suspect measles cases are tested for measles IgM antibody, excluding cases epidemiologically linked to a laboratory confirmed case from the denominator
Indicators for Measles Elimination Recommendations from EMR-TAG, 2006 • Adequacy of epidemiologic investigation* • Indicator: > 80% of suspect measles cases have an adequate epidemiologic investigation*. • Adequacy of laboratory testing • Indicator: > 80% of measles virus outbreaks and chains of transmission chains (outbreaks) have sufficient* samples for viral isolation • *An adequate investigation includes at a minimum the suspect cases with all of the following data elements; date of rash onset, specimen collection, date of specimen collection, vaccination status, date of last vaccination, age, and district)
Completeness of Reporting to Regional Office, Countries Reporting on a Monthly Basis, 2006 Palestine Bahrain Reporting on a timely basis (n=16) Delayed reporting (n=4) Inconsistent/not reporting (2 countries)
Suspect Cases+ per 100,000 in EMR, Jan-Dec-2006* Proposed regional target 2/100,000 + Suspect cases – lab and epi confirmed cases * Adjusted for annualized rate
Serologic Testing of Suspect Cases (Jan-Dec ’06, EMR)Indicator: > 80% of suspect cases with testing Palestine Bahrain > 80% of suspect cases (10 countries) 50-80% (3 countries) < 50% (7 countries) Not reporting (2 countries)
Adequacy of Epidemiologic Investigation, Jan-Dec ’06 EMR Indicator: >80% of measles case reports with complete investigation Palestine Bahrain > 80% (6 countries) 50-80% (5 countries) < 50% (6 countries) Not reporting (5 countries)
Recommended Criteria for Measles Elimination EMR-TAG, 2006 • Measles incidence of < 1 confirmed case per million per year, excluding cases confirmed as imported. • All districts with > 90% vaccination coverage for the first dose of measles vaccine and 95% coverage national coverage for the second dose. • 90% of outbreaks are < 10 cases in size • Epidemiologic and laboratory data indicate that measles viruses are imported.
Measles Cases per Million in EMR, Jan-Dec-2006* * provisional
MCV1 Coverage* Indicator: > 90% coverage in all districts Palestine Bahrain MCV1 > 90% in all districts (7 countries) MCV1 > 80% in all districts (2 countries) MCV1 > 50% in all districts (4 countries) MCV1 < 50% in some districts (8 countries) * Based on 2005 JRF, data is unavailable for Lebanon
Summary • Considerable progress in mortality reduction • Pak campaign will reduce further • Few countries are close to elimination • Several countries with large outbreaks • Failure of “keep-up” strategies • SIAs are playing an important role to achieve elimination
Summary • Surveillance is improving • Impact on program activities • Countries have accepted agreed upon indicators • RTAG will address issue of “certification”
Priority Activities • Advocacy • Raising awareness of national health authorities • Development of country-level TAGs • Certification process? • Surveillance • Revisit regional reporting format • Outbreak surveillance • Source of infection • Genotyping • Achieving high population-based immunity • Better monitoring of routine EPI data • Achieving and monitoring high MCV2 coverage • Monitoring susceptibility profiles at sub-national levels
EMR MCV Coverage and Percent of Games Won-Chicago Cubs, 1995-2006