Download
1 / 31
480 likes | 1.45k Vues
Autoimmune Thrombocytopenia (Idiopathic Thrombocytopenia Purpura, ITP). Autoimmune Thrombocytopenia. Acquired disorder Platelet autoantibodies destroy host and transfused platelets More frequently detected with routine testing using automated cell counters

E N D
Autoimmune Thrombocytopenia(Idiopathic Thrombocytopenia Purpura, ITP)
Autoimmune Thrombocytopenia • Acquired disorder • Platelet autoantibodies destroy host and transfused platelets • More frequently detected with routine testing using automated cell counters • Important to recognize a subgroup of mild, asymptomatic patients who require no treatment
Autoimmune Thrombocytopenia Age and Sex Distribution Data redrawn from Beutler, E, Lichtman, MA, Coller, BS, et al, Williams Hematology, 5th ed. McGraw-Hill, New York, 1995
Autoimmune ThrombocytopeniaRelationship of Bleeding to Platelet Count 1 = minimal bleeding after trauma 2 = spontaneous, self limited 3 = spontaneous, needing Rx 4 = severe, life-threatening Data from Lacy, JV, Penner, JA, Semin Thromb Haemost 1977;3:160
Autoimmune ThrombocytopeniaBleeding Manifestations • None in some patients • Petechiae and ecchymoses > menorrhagia>GI >> intracranial bleeding • Risk of intracranial hemorrhage <1% • Risks may be greater in elderly due to comorbidity • Oral bleeding and widespread skin bleeding (“wet purpura”): generally, an indicator of increased risk of serious bleeding
Autoimmune ThrombocytopeniaDiagnosis • A diagnosis of exclusion • No clinically apparent associated conditions that may cause thrombocytopenia • Isolated thrombocytopenia, with otherwise normal blood counts, including examination of peripheral smear
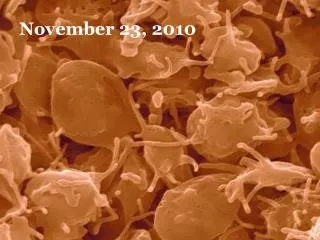
I.T.P.: Megathrombocytes Normal Platelet Number & Size
Autoimmune ThrombocytopeniaDiagnosis • No implicated drugs • especially heparin, quinine, quinidine, sulfonamides, b-lactams, fludarabine • No splenomegaly • No evidence of sepsis • Normal coagulation tests • No RBC microangiopathy
Autoimmune ThrombocytopeniaDiagnosis • Usually idiopathic, but may be secondary to: HIV-1, CLL/NHL, other autoimmune diseases • Further testing: • HIV-1 in patients with risk factors • Bone marrow with karyotype in older patients to exclude myelodysplasia • Thyroid function testing to exclude infrequent coincidence of autoimmune thyroid disease
Historical Background • 1951: Harrington, et al showed an “antiplatelet factor” in plasma caused ITP. • 1965: Shulman, et al identified a 7S IgG anti-platelet aby in pts’ plasma. • 1975: Dixon, et al first measured platelet associated IgG on plts. • 1987 Macmillan, et al in US and Kiefel, et al in Germany described new assays for platelet associated autoabys. Harrington, et al., J Lab Clin Med 38:1, 1951
Immunopathogenesis of ITP IgG or IgA autoabys B cell-derived plasma cell GPIa/IIa Fc-mediated R.E. Cell Clearance GPIV, V GPIIb/IIIa GPIb/IX IFNg Platelet IL-10 IL-2 CD4 auto- reactive T cells gd Tcells
Natural History of ITP • Stasi, et al (Am J Med 1995; 98:436) • 208 adults with ITP followed for median of 92 months: • 42% had pltc > 50,000 and were not treated • Spontaneous remission rate: 9% • At last follow-up in 95 treated pts, 43 in CR, 52 still being treated • 5 deaths attributable to thrombocytopenia
Autoimmune Thrombocytopenia General Treatment Philosophy • Treatment should be restricted to pts with moderate (20-40K/mL) or severe (<20K/mL) thrombocytopenia. • Goal is to achieve a safe platelet count. • Treatment should be limited in duration once a response is obtained.
Initial Treatment of ITPGlucocorticoids • Prednisone, 1 mg/kg/d • Response expected by 2 weeks. • Duration of therapy determined by platelet count response. Taper slowly (4-6 wks) • Complete response in 40%. • Most responders have recurrence with tapering. • Sustained response for 6 months in only 20%. • Other therapies will be needed in most
Initial Treatment of ITPInitial Treatment with High Dose Dexametasone Cheng, Y, Wong, R.S.M., Soo, O.Y., et al. NEJM 2003; 349:831-835. • 157consecutive patients • 125 eligible with initial pltc mean of 12,200/mL given dexamethasone, 40 mg/d x 4 days • Good initial response (pltc increase of at least 30,000/mL) in 106/125 (85%) with mean pltc increase by at least 20,000/mL by day 3 and mean pltc increase to 101,400 ± 53,200/mLby 7 days after treatment • 53 (50%) had sustained response • 53 (50%) had relapse within 6 mos., most within first 3 mos. • Pltc < 90,000/mL on day 10 associated with high relapse risk. • Treatment well tolerated.
Steroid-Refractory ITP Splenectomy • Traditionally considered second-line treatment for adults with ITP who fail steroids. • Opinions vary as to timing of splenectomy. • Approximately 50-65% will achieve a normal platelet count which is sustained. • CRs are achieved by week 2. • Only consistent predictor of response is age. • Response to steroids, IVIG, anti-D are all inconsistent predictors of response.
Cumulative Response to Splenectomy Age < 40 Age < 40 Age > 40 Fabris, F, et al, Br J Haematol 2001;112:637
Steroid Refractory ITPMorbidity from Splenectomy • Greatest morbidity in the obese, elderly and those with comorbidities. • Morbidity as high as 26% in one series of 78 splenectomized ITP pts. • Morbidity less with laparoscopic approach. • Sooner ability to eat liquid diet • Less pain • Quicker discharge • Operative time no shorter • Mortality from sepsis = 0.73 per 1000 pt.yrs.
Other Initial Treatments IVIG • Especially useful for bleeding emergencies in pts with “acute” ITP to transiently increase platelet count. • Godeau, B, et al Br J Haematol 1999;107:716 randomized, prospective, multicenter (n = 36) • 0.5 or 1.0 g/kg on day 1, up to 2g/kg by day 4 if needed • Increase in platelet count >80,000: 6% and 28% on day 2; 24% and 67% on day 4; overall response to 2 g/kg by day 7: 78% • Transient, reversible side effects: hypertension, chills, emesis, hypotension; rarely, renal failure
Other Initial Treatments Anti-(Rh)D • Effective only in Rh-positive patients. • Not expected to induce long-term CR • Dose: 50-75 mg/kg I.V. • Response rate in one series* was 70% with responses lasting >21 days in 50%. • Mild hemolytic anemia occurs. If RBC transfusion needed, use Rh neg. cells. Scaradavou, A, et. al. Blood 1997;89;2689
Other Initial TreatmentsNovel Approaches • Evaluate for and treat H. pylori infection: Gasbarrini, et al* • High rate of H. pylori infection among their ITP pts • 8 of 11 who had eradication of infection had significant increase in pltc at 2 and 4 months; 6 of 8 had disappearance of autoantibody (p<0.003) • Others** have been unable to duplicate results • Splenic irradiation and splenic embolization * Gasbarrini, A., et al, Lancet 1998; 352:878 (Sept.) ** Jarque, I., et al, Br J Haematol 2001; 115:1002-1003
Chronic Refractory ITP • ITP has persisted for > than 3 months • Failure to respond to first line therapy and splenectomy • Platelet count <30,000/mL • Best treatment uncertain
Chronic Refractory ITPMultiple Therapeutic Approaches • High dose dexamethasone • Cytoxan, vincristine, prednisone (CVP) • Azathioprine • Danazol • Vinblastine • Interferon a • Cyclosporin • Accessory splenectomy • Rituximab (chimeric anti CD-20) • Mycophenolate mofetil • High dose cyclophosphamide/autologous PSCT
Chronic Refractory ITPChimeric Anti-CD20 • Four reported series in literature as of 8/03 • Stasi, et al* • 25 pts with refractory primary ITP • Resistant to 2-5 regimens, 8 splenectomized • Complete response (pltc>100K) in 5 • Partial response (pltc 50-100K) in 3 • Minor response (pltc <50K, but stable) in 3 • Overall response = 52% • 7 with sustained responses (>6 months) • 2 relapses remitted with retreatment *Stasi, R, et al, Blood 2001;98:952
Chronic Refractory ITPLong-term Outcomes • 183 patients (158 adults, 25 children)* • 47 refractory to splenectomy prospectively followed for median of 7.5 yrs • 12 with moderate thrombocytopenia, untreated • 35 treated with median of 2 salvage treatments • 36 (77%) reached durable pltcs >100K • 9 with no treatment • 27 with low dose steroids or azathioprine • In 6, pltc. remained at 35-100K • 5 remained severely thrombocytopenic • 3 adults and 1 child died of bleeding Bourgeois, E, et al. Br J Haematol 2003;1079-1088
Chronic Refractory ITP(Modified from George, JN, et al NEJM 1994;331:1207)
I.T.P. “Let the treatment fit the patient.” --James N. George, M.D. (NEJM 2003; 349:903-905