Download
1 / 17
180 likes | 207 Vues
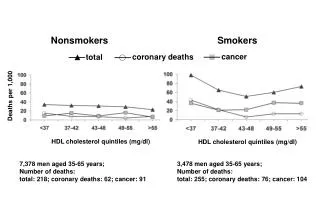
Learn about the impact of HDL-cholesterol and apoA-I on atherosclerosis regression in a comprehensive review by Prof. Erik Stroes from Amsterdam, Netherlands. Discover the role of exogenous cholesterol, VLDL, LDL, chylo-microns, and peripheral tissues like the intestine and liver in the process. Explore how HDL influences cardiovascular risk via reverse cholesterol transport. Uncover the association between HDL-c concentration and cardiovascular risk based on cohort studies and meta-analyses. Understand the latest findings on drug-induced increases in HDL-c and their effects on cardiovascular events. Explore novel therapies targeting apoA-I and HDL for plaque regression and atherosclerosis reversal. Delve into ongoing clinical trials investigating the potential of elevating HDL-c and apoA-I levels in reducing cardiovascular risk.

E N D
HDL-cholesterol versus apoA-Iand Atherosclerosis Regression Prof. Erik Stroes AcademicMedical Centre Amsterdam, The Netherlands
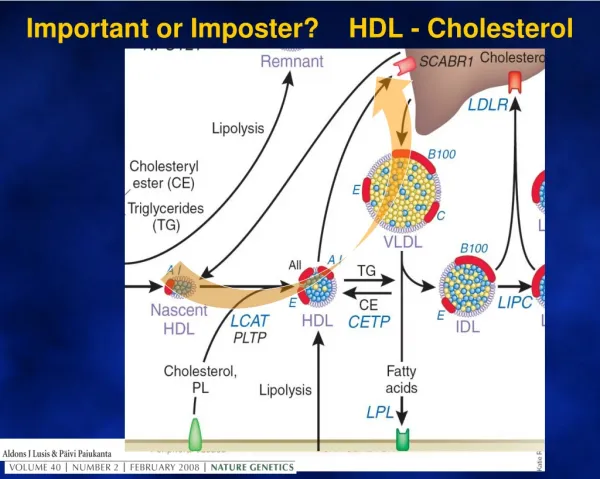
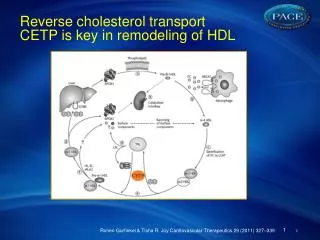
Exogenous cholesterol VLDL LDL Chylo-microns PERIPHERAL TISSUES INTESTINE LIVER Bile excretion HDL HDL-c decreases CV-riskvia ‘Reverse cholesterol transport’ Risk 4.0 4.0 3.0 2.0 2.0 MACROPHAGE 1.0 1.0 0 1.68 0.65 1.17 HDL-c (mmol/L) Kannel WB AJC 52, 1983 – Framingham Study
HDL-c concentration and CV-riskNo association ‘genetic’ HDL-c increase and risk Cohort Atherosclerosis Risk in Communities Study Copenhagen City Heart Study Malmo Diet and Cancer Study, Cardiovascular Cohort Framingham Heart Study Heart Professionals Follow up Study Danish Diet, Cancer, and Health Study Meta-analysis of cohort studies Per 0.03 mmol/L (1 mg/dL) increase in plasma HDL-c Per 0.39 mmol/L (15 mg/dL) increase in plasma HDL-c Epidemiology OR / 0.03 mmol/L HDLc increase Genetics OR / 0.03 mmol/L HDLc increase 0.97 (0.96-0.98) 0.98 (0.98-0.99) 0.97 (0.96-0.98) 0.96 (0.94-0.98) - - 0.98 (0.97-0.98) 0.70 (0.66-0.74) 7x10-18 6x10-13 1x10-6 4x10-6 - - 4x10-36 4x10-36 0.96 (0.86-1.07) 1.09 (0.95-1.26) 0.82 (0.66-1.01) 1.17 (1.00-1.37) 1.84 (0.39-8.62) 1.05 (0.79-1.41) 1.02 (0.95-1.09) 1.28 (0.46-3.61) 0.44 0.21 0.06 0.06 0.16 0.71 0.64 0.64 Voight, Lancet 2012
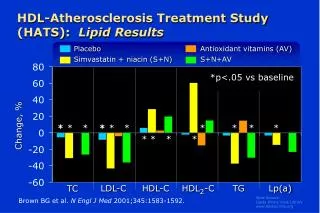
HDL-c concentration and CV-riskNo association ‘drug-induced’ HDL-c increase and risk • ILLUMINATE Torcetrapib: • HDLc +72% : CV-death OR +1.25 • DALOUTCOMES Dalcetrapib: • HDLc +35% : CV-events no change • HPS2-THRIVE Nicotinic acid: • HDLc +15-25% : CV-events no change • Meta-analysis Briel et al • HDLc +2-15% : CV-events no change • HDL-c change no longer valid as surrogate • for future CV-risk. Barter, New Engl J Med 2007; Schwartz GG, New Engl J Med 2012 Eur Heart J 2013; Briel, BMJ 2009
HDL-c and Reverse cholesterol transportNo association between HDLc and fecal chol. excretion • HDL-c concentration no longer valid as surrogate • for RCT capacity. Broussea, ATvB 2005
Decreased ‘Tissue cholesterol efflux’in apoA-I/L178P heterozygotes Holleboom, Stroes J Lipid res 2013
Increased ‘Vessel-wall thickening’in ABCA1 & LCAT- heterozygotes LCAT heterozygotes ABCAI heterozygotes Mean wall area outer wall area Duivenvoorden, Stroes, JACC 2010; Bochem, Stroes, J Lip Res 2013
Number of HDL particles more relevantthan HDL-c concentration Mackey et al., JACC 2012
apoA-I increase and RCTeffect of rHDL particle infusion (≈ 45mg/kg) AfterInfusion Before Infusion Bile Acids 400 Neutral Sterols HDL-C (mg/dl) 41±7 35% peakIncrease 300 Intestinal Excretion mg/day 200 100 0.0 SG GG LM IN Eriksson, Circ 1999
apoA-I increase and Plaque regressioneffect of rHDL particle infusion (40mg/kg) on peripheral atheroma Shaw, Circ Res 2008
apoA-I and Plaque regressionEffect of ApoAI milano on coronary atheroma P=0.02 REVERSAL ASTEROID APOA-1 Milano 4 4 2.7* 2 Median change in TAV (%) -0.3† -0.8 -4.2 0 Prava 40 mg 18 months Atorva 80 mg 18 months -2 Rosuva 40 mg 24 months -4 ApoA-1 Milano 5 weeks From no change to regression Progression Nissen SE et al. JAMA. 2003 and 2004
apoA-I and Plaque regressionrHDL& delipidated HDL and coronary atheroma Reconstituted HDL (CSL-111) Delipidated HDL (LS-001) Tardiff, JAMA 2007; Waksman, JACC 2010
New apoA-I therapiesCER-001 • composed of recombinant human Apolipoprotein A-I and phospholipid containing Sphingomyelin and dipalmitoyl phosphatidylglycerol • reconstituted charged pre-beta High Density Lipoprotein, mimicking biological properties of natural HDL CER-001: recombinant human apoA-I preB HDL particle
Preliminary results SAMBA studyCER-001 infusion in Subjects with Familial HDL-C deficiency Trial design: Baseline Evaluations Lipoprotein profile Cholesterol Flux MRI Initial Dosing Period CER-001 Day 1 Lipoprotein profile PK and PD Cholesterol Flux Induction Period CER-001 q3 days Day 8 through Day 29 Lipoprotein profile PK and PD MRI Day 29 Maintenance Period CER-001 q2 weeks Week 6 through Week 24 Final Dosing Period CER-001 Week 26 Lipoprotein profile PK and PD MRI Study Drug Dosing Final dose First dose CER-001 8mg/kg Infusions every 3 days CER-001 8mg/kg, Day 1 to Day 29, 9 doses total Infusions every 2 weeks CER001 8mg/kg, 10 doses • Methods: • Safety & lipid profiles • Cholesterol flux: 2H4-sitostanol (oral)13C2-cholesterol (iv) • Vessel wall dimension: 3T-carotid & aorta MRI
Summary Both HDL-chol & apoAI are inversely related to CVD-risk Recent drug trials & genetic studies challenged the protective role of HDL Novel concept:HDL particle number better predictor of CV risk? CER-001, a recombinant human ApoA-I particle: Promotes plasma efflux capacity Promotes fecal cholesterol excretion Reduces carotid wall thicknessin patients with genetic low-HDLc levels Ongoing clinical trials with HDL-c & apoAI elevators will help us determine the value of HDL vs. ApoA-I therapy