Download
1 / 9
120 likes | 345 Vues
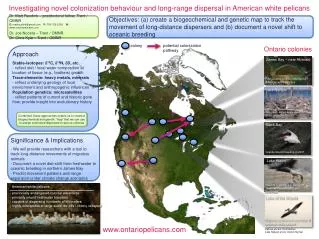
ESC 2013. European guidelines on the management of stable c oronary artery d isease. Key points & new position for Ivabradine and Trimetazidine.

E N D
ESC 2013 European guidelines onthe management ofstable coronary artery disease Keypoints & new position for Ivabradine and Trimetazidine Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
Aims to focus on • To obtain relief of angina symptoms theguidelines advise: Short-acting nitrates to provide immediate relief of angina symptoms. Anti-ischemic drugs like -blockers, CCBs, Trimetazidine, Ivabradine… Lifestyle changes, regular exercise training and patient education. • To prevent the occurrence of cardiovascular events theguidelines advise: To reduce the incidence of acute thrombotic events and the development of ventricular dysfunction by pharmacological or lifestyle interventions. A combined pharmacological and revascularization strategy in patients with severe lesions in coronary arteries. Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
Medical management of SCAD patients Event prevention Angina relief 1st line • Lifestyle management • Control of risk factors Short-acting nitrates, plus • β-blockers and/or CCB • Aspirin (if intolerance, consider clopidogrel) • Statins • Consider ACE inhibitors or ARBs 2nd line Ivabradine Long-acting nitrates Nicorandil Ranolazine Trimetazidine Chairmen opinion:* “We recommend the old drugs as first line treatment because they are cheap, effective and available everywhere.” + consider angio → PCI-stenting or CABG “We have roughly the same level of evidence for all of the second line drugs and we recommend that physicians also choose according to what is available in their country.” Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003. *New ESC Guidelines published on stable coronary artery disease. Eur Heart J. 2013;34:2927-2930.
Medical management of SCAD patients Event prevention Angina relief 1st line • Lifestyle management • Control of risk factors Short-acting nitrates, plus • β-blockers and/or CCB • Aspirin (if intolerance, consider clopidogrel) • Statins • Consider ACE inhibitors or ARBs 2nd line Ivabradine Long-acting nitrates Nicorandil Ranolazine Trimetazidine Chairmen opinion:* About revascularization, chairmen hopes that “guidelines will shift physicians’ practice so that they consider optimal medical treatment as their first course of action in stable CAD patients”. + consider angio → PCI-stenting or CABG Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003. *New ESC Guidelines published on stable coronary artery disease. Eur Heart J. 2013;34:2927-2930.
Specific patient profiles • Women • Women more frequently have CAD with stable angina and no obstructive coronary disease. • Women are more likely to have complications from revascularization. • Diabetic patients • Need different risk factor management. • Older patients • High-risk group with higher mortality and higher rates of myocardial infarction. • Usually undertreated, receiving less drugs. • Difficult diagnosis due to atypical symptoms. • Higher risk of complications during and after coronary revascularization. • Comorbidities/intolerance • Depending on comorbidities/tolerance, it is indicated to use second-line therapies as first-line treatment in selected patients. Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: the task force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
Therapy to prevent MI and death • Aspirin • Low-dose aspirin is the drug of choice in most cases and clopidogrel may be considered for some patients. • Statin • TargetLDL-C: <1.8 mmol/L and/or >50% reduction if the target level cannot be reached. • Renin-angiotensin-aldosterone system blockers • ACE inhibitors are recommended for the treatment of patients with SCAD, especially with coexisting hypertension, LVEF ≤40%, diabetes, or chronic kidney disease, unless contra-indicated. • ARBs are recommended as an alternative therapy for patients with SCAD when ACE inhibition is indicated but not tolerated. Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
New ESC guidelines and Ivabradine “Adding ivabradine 7.5 mg twice dailyto atenolol therapy gave better control of heart rate and anginal symptoms.” “In 1507 patients with prior angina enrolled in the Morbidity-Mortality Evaluation of the If Inhibitor Ivabradine in Patients With Coronary Artery Disease and Left Ventricular Dysfunction (BEAUTIFUL) trial, ivabradine reduced the composite primary end point of CV death, hospitalization with MI and HF, and reduced hospitalization for MI. The effect was predominant in patients with a heart rate 70 bpm.” “Ivabradine is thus an effective anti-anginal agent, alone or in combination with β-blockers.” Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
New ESC guidelines and Trimetazidine “Trimetazidine is an anti-ischemic metabolic modulator, with similar anti-anginal efficacy to propranolol in doses of 20 mg thrice daily.” “Trimetazidine (35 mg twice daily) added to β-blockade (atenolol) improved effort-induced myocardial ischemia, as reviewed by the EMA in June 2012.” In diabetic persons, Trimetazidineimproved HbA1c and glycemia, while increasing forearm glucose uptake.” Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.
Conclusion • ESC Guidelines highlighted two aims for the pharmacological management of stable CAD patients: obtain relief of symptoms and prevent cardiovascular events. • CAD patients should all receive aspirin and a statin, plus an ACE inhibitor in case of comorbidities. • -blockers or CCBs should be prescribed as first-line treatment to reduce angina. • Ivabradine and Trimetazidine(as well as long-acting nitrates, nicorandil and ranolazine) are recommended second-line, in combination with first-line treatment, in patients remaining symptomatic. • Physicians should consider optimalmedical treatment before revascularization procedures. Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease: The Task Force on the management of stable coronary artery disease of the European Society of Cardiology. Eur Heart J. 2013;34(38):2949-3003.