Bone Density Analysis
Bone Density Analysis. Information from Clinical Imaging with Skeletal, Chest and Abdomen Pattern Differentials By Dennis M. Marchiori and web search on May 17, 2007. Methods to Evaluate Bone Mineral Density. Bone mineral density measurements can be assessed by: Radiographs

Bone Density Analysis
E N D
Presentation Transcript
Bone Density Analysis Information from Clinical Imaging with Skeletal, Chest and Abdomen Pattern Differentials By Dennis M. Marchiori and web search on May 17, 2007.
Methods to Evaluate Bone Mineral Density • Bone mineral density measurements can be assessed by: • Radiographs • Quantitative Computed Tomography (QCT) • Single Photon Absorptiometry (SPA) • Dual Photon Absorptiometry (DPA) • Dual Energy X-ray Absorptiometry (DEXA) • Ultrasound
Bone Mineral Analysis • Quantitative Computed Tomography is the most accurate method but there are problems associated with: • High radiation dose from computed tomography • High cost due to cost of equipment. • Dual Energy X-ray Absorptiometry (DEXA) is the most widely used method.
Dual Energy X-ray Absorptiometry • DEXA is very in evaluating patients at risk of osteoporosis before complications such as bone fragility or fractures occur. • DEXA can also be used for follow up studies to track progress or response to treatment. • Follow up exams should be done on the same unit.
Image Production SPA • Single Photon Absorptiometry (SPA) uses a single energy beam of radiation to measure the bone density of the peripheral skeleton, usually the calcaneus or distal radius. • Bone density is determined by the attenuation of the beam. • Measurement extrapolated to estimate density in the spine or hip. • Correlation of the peripheral bone density and spinal density is moderate at best leaving room for error.
Image Production: DPA and DEXA • Dual Photon Absorptiometry (DPA) uses radiation beams of two energy levels using a radionuclide to measure the bone density of the lumbar spine and hip. • Dual Energy X-ray Absorptiometry (DEXA) is an improvement to DPA technology using an x-ray tube as the source of radiation instead of a radionuclide.
Image Production: DEXA • DEXA uses to separate energy levels and depends upon the differential absorption of the tissue to create the measurement of bone density. • DEXA examinations are generally much quicker than DPA studies. • First DEXA machines used a pencil beam, newer units use a fan beam.
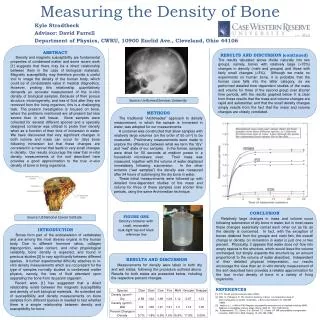
Patient Experience: DEXA • The patient is asked to lie supine on a couch under the x-ray tube. The patient will generally not be asked to change into a gown. • The operator will center the tube over the spine and/or upper femora. The scan will take about 10 to 20 minutes for a basic BMD examination. The patient will be asked to remain as still as possible for the exam.
Clinical Applications • New developments in DEXA are leading to major improvements in diagnosing osteoporosis, more accurately determining future fracture risks and most recently diagnosing cardiovascular disease. • New fan beam machines can detect vertebral fractures with a fast, low dose lateral scans of the vertebra from T4 to L4 in as little as 10 seconds.
Clinical Applications • Vertebral fractures are the most common fracture with osteoporosis and an indication for treatment irrespective of the BMD. However without a diagnostic test such as fan beam DXA systems, as many as 75% of vertebral fractures would never come to clinical attention. • DEXA is the tool of choice for detection of osteoporosis.
Osteoporosis Overview • Osteoporosis is a serious, but not fully understood disease. • Estimated 10,000,000 American women suffer from osteoporosis. • Osteoporosis causes 1.5 million fractures in the U.S. • Osteoporosis fractures cost $13.8 billion annually.
Osteoporosis Overview • Osteoporosis is the direct cause for 500,000 hospital admissions, 2.6 million doctor visits and nearly 180,000 nursing home admissions. • Osteoporosis is a “silent disease. In the US, 4 times as many men and nearly 3 times as many women have the disease than report having the condition.
Osteoporosis Overview • All fractures associated with significant morbidity and mortality but hip fractures are particularly traumatic. 20% of women who suffer a fractured hip die within the first year.
Indications for BMD • The International Society of Clinical Densitometry has identified those patients most likely to benefit from BMD screenings as: • Women 65 years and older • Postmenopausal women under 65 with risk factors. • Men 70 years and older • Adults with fragility fractures • Adults with disease associated with low bone mass. • Adults taking medications associated with low bone mass. • Patients being treated for osteoporosis.
Indications for BMD • Risk factors for osteoporosis include: • Paternal history of hip fracture • Smoking • Cortical steroids use • Alcohol abuse • Clinical disorders related to low BMD • Hyperparathyroidism • Hyperthyroidism • Malabsorption
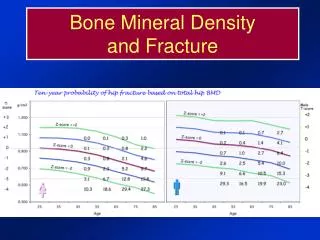
DEXA T-scores • T-scores are calculated by subtracting the patient’s bone mineral density from a reference range of peak bone density in a young person of about 35 years of age. • The value is then divided by the standard deviation of the reference standard to produce the T-score.
Classification of BMD Assessed by DEXA T-scores • In general terms, there is about a 10% loss of bone density for every standard deviation change in T score. • T-score of -1 or higher = Normal Bone density • T-score of -2.5 to -1 = Osteopenia • T-score below -2.5 = Osteoporosis • T-score below -2.5 and fragility fracture = severe osteoporosis
T-score Predictor of Fracture Risk • The risk doubles for every standard deviation change. • T-score of 0 has average risk for a normal 40 year old. • T-score of -1 has twice the risk • T-score of -2 has four times the risk factor • T-score of -3 has eight times the risk.
T-scores and Z-scores • There is a strong correlation between the occurrence of low bone mineral density and prediction of fracture occurrence. For each increase in T-score, the risk of fracture doubles. • Z-scores are used to compare the patient’s bmd with persons of matched age, gender and ethnicity.
Z-scores • Z-score of 0 indicates that half of the population has greater bone density. • Z-score of “-1”, 84% of population has better bone density • Z-score of “-2”, patient is at the 2nd percentile and 98% of the population has greater bone density. • A score of less than -1.5 raises the suspicion that something other than age is accounting for the low bone mineral density.
Vertebral Fracture Assessment • Vertebral fractures are the most common osteoporosis fracture but only about 25% of the fractures come to clinical attention. • Women with vertebral fractures have shown to have a five fold increase in their risks for subsequent fracture and a two fold increase in the likely hood of a hip fracture.
Vertebral Fracture Assessment • One of every 5 women who have an incident with a vertebral fracture will have a subsequent fracture within the next year. • Modern fan-beam machines can perform VFA of the T-4 to L-4 vertebrae in as little as 10 seconds and with exposure at 1/15th that on conventional x-ray.
Vertebral Fracture Assessment • For DEXA machines with a rotating C-arm, the lateral scan can be done without moving the patient from the supine position. • By combining DEXA and VFA, the two strongest risk factures for future fracture can be obtained on the same device with little added exam time.
Vertebral Fracture Assessment • VFA has the potential to greatly improve the diagnostic accuracy in identifying women who are eligible for treatment. • In recent studies for women over age 65, 20 – 25% have vertebral fractures that would not qualify for treatment from the BMD alone.
Hip Structural Analysis • Hip structural analysis is a program for computing the structural properties of various cross sections of the proximal femur using 2D DXA scans. HSA algorithms are able to calculate bone strength in the two dimensions projected on the scan.
Hip Structural Analysis • The natural extension of HSA is to consider the femur as the 3D object that it is and to calculate the strength in 3 dimensions. • The nest generation of DXA imaging will use rotating c-arm features to make multiple images that can be combined to form a 3D tomographic representation of the hip.
Hip Structural Analysis • The low dose tomographic assessment is expected to become the ultimate clinical tool for the diagnosis of osteoporosis. • Not only will it give a more accurate picture of bone density but also the geometry and underlying strength of the bone.
DXA and Heart Disease and Stroke • Recently the FDA cleared on manufacture of DXA systems for the evaluation of abdominal aortic calcification which is strongly associated with cardiovascular disease. • The risks of CVD and stroke increase with age. 39% of the female deaths in the US occur from CVD.
DXA and Heart Disease and Stroke • With proper positioning, which is automatically accomplished with the rotating c-arm featured in some DXA machines, Abdominal Aortic Calcifications can be seen in the same scans used for VFA. • AAC seems to be a particularly strong risk factor in postmenopausal women, the same population benefiting from VFA.
End of Lecture Return to Physics Lecture Index