The New FIGO Staging for GTN
580 likes | 1.79k Vues
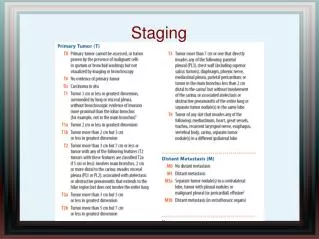
The New FIGO Staging for GTN. Tally Levy Division of Gynecologic Oncology Department of Obstetrics & Gynecology Wolfson Medical Center. ONCOLOGY. Staging: Clinical/surgical Determines prognosis Facilitates treatment decisions Enables a comparable reporting of data

The New FIGO Staging for GTN
E N D
Presentation Transcript
The New FIGO Staging for GTN Tally Levy Division of Gynecologic Oncology Department of Obstetrics & Gynecology Wolfson Medical Center
ONCOLOGY • Staging: • Clinical/surgical • Determines prognosis • Facilitates treatment decisions • Enables a comparable reporting of data • Allows objective comparison of treatment results • TNM • FIGO (International Federation of Gynecology and Obstetrics) • 113 countries or territories.
Gestational Trophoblastic Neoplasia - GTN The Hammond Clinical Classification The WHO (Bagshow) Classification Old Revised The FIGO Classification New 2000
GTN • Confusion in terminology: • Gestational trophoblastic disease • Benign? Malignant? • Persistant GTD? • Gestational trophoblastic tumor • (GTD, invasive mole, choriocarcinoma) • Clinical choriocarcinoma (Japanese) • Gestational trophoblastic neoplasia (GTN)
GTN Treatment Criteria • Persistant GTD: • Treat early after 2 weeks hCG or 3 weeks plateau? • Wait longer? treat less patients! • Lung metastases: • To treat or not to treat? • Size & number cut-off?
Staging & Scoring SystemsOver the History • Morphological & histological classifications • Not in use because in most pts today there is no precise pathology • The decision to treat is usually made on hCG levels and clinical features • The International Union Against Cancer (UICC)- 1967 • Combined clinical + morphological criteria • An attempt to take into account the prognostic importance of both
Japanese Morphologic classification - 1967 to date If histopathologic diagnosis Is not available
1st FIGO Classification • Acording to Song et al 1981 from Beijing • Not universally accepted • Prognosis varied within stages • Prognosis dependent on certain clinical features • Leading to under-treatment & over-treatment Hancock BW, Best Prect & Res Obstet Gynecol 2003 Smith et al, Br J Obstet Gynecol 1993
Clinical Classifications • Berkowitz RS & Goldstein DP • New England Trophoblastic Disease Center • Harvard Medical School, Boston • Bad prognostic features (1965): • High hCG level • Duration of disease > 4 months • Brain and/or liver mets
Clinical Classifications • Berkowitz RS & Goldstein DP • New England Trophoblastic Disease Center • Harvard Medical School, Boston • Bad prognostic features (1965): • High hCG level • Duration of disease > 4 months • Brain and/or liver mets
The Hammond Clinical Classification • Based on NIH data • Became popular in the US • Not complicated • Immediate segregation of non-metastatic disease to single-agent treatment • Allows easy identification of patients needing multiple-agent chemotherapy
The Bagshawe Classification 1976 King's College Hospital Medical School, London 317 GTTs
Staging vs Scoring Systems • No agreement on which is best • None shown to be superior • WHO score more predictive for prognosis than FIGO • Both Hammond clinical classification and WHO equivalent for stratifying pts into low- and high-risk groups • Difficulties in applying certain scores: • Blood group data might be missing • Should the scoring system be applicable to non-metastatic disease? Hancock BW, Best Prect & Res Obstet Gynecol 2003 Soper JT, Obstet Gynecol 2006
Revised FIGO Staging • Mixed reaction from different centers • Reliably predicts treatment outcome • (Goldstein et al,J Reprod Med, 1998) • Close correlation between FIGO & WHO results reflected also in treatment results • (Ma et al, 1997, Chinese comparison in 207 pts) • 3 systems equally discriminate between low and high risk pts but Not all factors are independent • (soper et al, Obstet Gynecol 1994) • Multivariate analyses shows some variables discriminate unfavorable outcome. Variables comparable to the WHO score and better than the Hammond or FIGO system in predicting outcome • Lurain et al, Am J Obstet Gynecol 1991 • 1391 pts from the Brewer Trophoblastic Disease Center, Chicago
GTN • Too many scoring & staging systems • All based on retrospective data • Based on different variables • Impossible to compare prognostic & treatment results around the globe
Workshop Report Combining the staging system of the International Federation of Gynecology and Obstetrics with the scoring system of the World Heath Organization for Trophoblastic Neoplasia. Report of the Working Committee of the International Society for the Study of Trophoblastic Disease and the International Gynecologic Cancer Society E. I. Kohorn*, D. P. Goldstein†, B. W. Hancock‡, S. J. Kim§, J. R. Lurain¶, E. Newlands**, J. T. Soper†† & L. C. Wong‡‡ *Yale Trophoblast Center, New Haven, Connecticut, USA; †New England Trophoblast Center, Harvard Medical School, Boston, Massachusetts, USA; ‡Trophoblast Center, Sheffield, UK; §Catholic University School of Medicine, Seoul, South Korea; ¶Brewer Trophoblast Disease Center, Chicago, Illinois, USA; **Charing Cross Hospital, London, UK; ††Southeastern Trophoblast Center, Durham, North Carolina, USA; ‡‡Queen Elizabeth Hospital, Hong Kong, China
New 2000 FIGO Staging & Risk Scoring System • Low risk group: score of 6 • Single agent chemotherapy • High risk group: score 7 • Combination chemotherapy
New 2000 FIGO Staging & Risk Scoring System • Unanimously agreed that the basic FIGO stage I,II,III,IV would be retained • The modifiers of the revised FIGO (risk factors) be excluded and replaced by the WHO score • Stage 0 (HM with spontaneous resolution) will not be included
Modifications of the WHO scoring to be combined with FIGO stage a. The prognostic scores should be 0, 1, 2, 4 for individual risk factors. Hong Kong has agreed to upgrade their highest risk factor from 3 to 4 and Charing Cross and Sheffield agreed to allot 4 rather than 6 for their highest risk factor. The efficiency of this change has been confirmed by multivariate analysis. b. The ABO blood group risk factors are to be eliminated as their significance has not been confirmed. c. The risk factor for liver metastasis will be upgraded from 2 to the highest risk group, 4. Kohorn EI et al, Int J Gynecol Cancer, 2001
Modifications of the WHO scoring to be combined with FIGO stage d. For lung metastases, the number of metastases to be included in the count will require that each metastasis is equal or greater than 3 cm. e. It was unanimously agreed that placental site tumors will be reported separately from other gestational trophoblastic tumors as the clinical condition, management, and prognosis of the two are significantly different. Kohorn EI et al, Int J Gynecol Cancer, 2001
New 2000 FIGO Staging & Risk Scoring System - Weaknesses • No accounting for HM • No point to do staging procedures at initial diagnosis • Needs separate recording • Dynamic staging system?! • How to diagnose intra-abdominal, hepatic and brain mets? • Problematic in certain developing countries • Left to institutional preference • Diagnosis of lung metastases • All metastases visible on chest X-ray should be counted (not on CT) • Less pts will receive combination chemotherapy Kohorn EI, Int J Gynecol Cancer, 2001
96 pts with low-risk metastatic GTN • 102 pts with low-risk non-metastatic GTN • Retrospective assessment of lung findings by CT compared to CXR • No significant difference in need to change to 2nd line chemo or in time to remission if score changed by CT • CT scan of the chest used instead of CXR in GTN staging does not alter outcome
Acta Obstet Gynecol Scand. 2009;88(2):204-8. • Treatment of gestational trophoblastic neoplasia according to the FIGO 2000 • staging and scoring system: a 20 years' experience. • Wang KL, Yang YC, Wang TY, Cheng-Yen Lai J, Chen TC, Chang CL. • Department of Obstetrics and Gynecology, Mackay Memorial Hospital, Taipei, Taiwan, • Province of China. KL421229@ms6.hinet.net • OBJECTIVE: To reassess the efficacy of the Federation of Gynecology and Obstetrics • (FIGO) 2000 staging and risk factor scoring system in comparison to the original World • Health Organization (WHO) prognostic scoring system (1983) in a single-institute setting. • DESIGN: Retrospective review of the medical records of 89 patients with gestational • trophoblastic neoplasia. • SETTING: Mackay Memorial Hospital, Taipei, a regional referral center for northern • Taiwan, over a 20-year period. • METHODS: All selected patients were classified retrospectively by the original WHO • prognostic scoring system (1983) and the FIGO 2000 system.
Acta Obstet Gynecol Scand. 2009;88(2):204-8. • Treatment of gestational trophoblastic neoplasia according to the FIGO 2000 • staging and scoring system: a 20 years' experience. • Wang KL, Yang YC, Wang TY, Cheng-Yen Lai J, Chen TC, Chang CL. • Department of Obstetrics and Gynecology, Mackay Memorial Hospital, Taipei, Taiwan, • Province of China. KL421229@ms6.hinet.net • RESULTS: The correlation was 97%. Only two patients were classified as middle risk • group in the original WHO system (1983), but as high-risk group by the FIGO 2000 • system. • CONCLUSION: There was good correlation between the original WHO (1983) and FIGO • 2000 systems. Treatment outcomes by FIGO 2000 system were somewhat better than • By the original WHO classification.
J Reprod Med. 2008 Aug;53(8):615-22. Links • An evaluation of FIGO 2000: the first 5 years. • Okines AF, Morris R, Hancock BW. • Department of Medicine, The Royal Marsden Hospital, Sutton, Surrey, UK. • Prospective evaluation • N= 122 pts from one center • 107 pts scored as low risk • 15 high risk • 35.5% of the low risk group required salvage chemotherapy • No affect on survival
Discussion: • Increased need for 2nd line chemotherapy in low risk pts under the new system (38% of LR from 2000 vs 23% before) • In pts with a score of 6 63% required salvage chemotherapy • Most of them (18/19) had hCG levels of 105 IU/l
Discussion: • Pts with risk score of 6 should be considered for an early switch to salvage chemo • Consideration should be given to change the cut-off score of low-risk to 5 • Maybe by increasing the risk score allocated to the hCG level of 105 IU/l from 4 to 6 points
Conclusions • The New 2000 FIGO Staging & Risk Scoring System was made in order to organize the Babylon tower • It is a more precise tool of reporting GTN • Allows valid comparison of treatment results from different centers