Bell’s Palsy
110 likes | 786 Vues
Bell’s Palsy. Bell’s Palsy. Characterized by: Peripheral facial paralysis Acute benign cranial polyneuritis Acute disorder characterized by a disruption of the motor branches of cranial nerve VII on one side of the face. (in absence of stroke).

Bell’s Palsy
E N D
Presentation Transcript
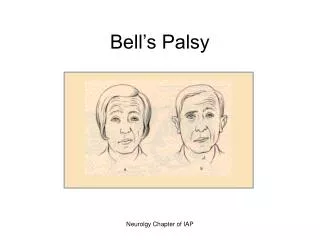
Bell’s Palsy Neurolgy Chapter of IAP
Bell’s Palsy • Characterized by: • Peripheral facial paralysis • Acute benign cranial polyneuritis Acute disorder characterized by a disruption of the motor branches of cranial nerve VII on one side of the face. (in absence of stroke) Neurolgy Chapter of IAP
Can affect any age group, though more common from 20-60. Etiology unknown; though reactivated herpes simplex may be involved. Reactivation causes edema, inflammation, ischemia, and eventual demyelination of the nerve, creating pain and alteration in motor and sensory function. Bell’s Palsy Neurolgy Chapter of IAP
Benign, with 85% of people recovering in 6 months-remaining 15% have some asymmetry of facial muscles Clinical manifestations Neurolgy Chapter of IAP
Clinical manifestations • Often accompanied by an outbreak of herpes vesicles in or around the ear. • Pain around or behind the ear • Fever, tinnitus, hearing deficits • Flaccidity of the affected side of the face with drooping of the mouth accompanied by drooling DT paralysis of the facial nerve (motor branches) Neurolgy Chapter of IAP
Clinical manifestations • Inability to close the eyelids, with an upward movement of the eyeball when closure is attempted; lower lid may turn out • Wide palpebral fissure (opening between eyelids) • Flattening of the nasolabial fold • Inability to smile, frown, or whistle • Unilateral loss of taste • Altered chewing ability; loss of or excessive tearing Neurolgy Chapter of IAP
Complications • Psychological withdrawal DT changes in appearance,malnutrition or dehydration, mucous membrane trauma, corneal abrasion, muscle stretching, and facial spasms and contractures. Neurolgy Chapter of IAP
Diagnostic Studies • Diagnosis made on basis of symptoms in the absence of other causes of paralysis such as stroke. • No definitive test • EMG may determine nerve excitability or absence Neurolgy Chapter of IAP
Therapeutic Management • Corticosteroids- drug of choice • Prednisone may be started immediately! • Best if initiated before paralysis is complete • Taper off over 2 weeks • Decrease edema and pain Analgesics may be needed for pain Antivirals : Acyclovir (Zovirax) and Famvir because HSV is implicated in 70% of cases. See Lewis 1719-1720- Nursing Implementation Neurolgy Chapter of IAP