Download
1 / 51
572 likes | 2.53k Vues
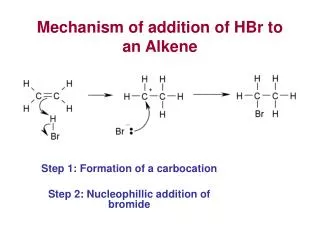
Delayed gastric emptying after Roux-en-Y reconstruction after gastrectomy : Mechanism and management. Dr R Botha Moderator: Prof Mieny. Background:. Cesar Roux described the Roux-en-Y gastrojejunostomy in 1897.

E N D
Delayed gastric emptying after Roux-en-Y reconstruction after gastrectomy: Mechanism and management. Dr R Botha Moderator: Prof Mieny
Background: • Cesar Roux described the Roux-en-Y gastrojejunostomy in 1897. • Procedure was abandoned because of the high incidence of marginal ulceration (simultaneous vagotomy was not performed). • 1950’s it was used in patients with partial gastrectomy and Billroth I or II reconstruction who presented with alkaline reflux gastritis or dumping. • In 1975 Davidson and Hersh reported on long term follow-up of patients after Roux-en-Y who presented with symptoms of delayed emptying from gastric remnant and Roux limb.
Gastric emptying: • Normal gastric emptying is controlled by an intact vagus nerve and a normally functioning antropyloric mechanism. • Fundus of the stomach maintains its tone under vagalinnervation that allows emptying of liquids. • Solid emptying is dependent on an innervated antrum and rhythmical contractions to move solid particles and liquid across the pylorus. • Duodenal receptors sensitive to pH and osmolality are responsible for feedback mechanism regulating antropyloric emptying.
Total gastric vagotomy: • Total gastric denervation • 80-90% decrease in basal acid output and a 50-60% decrease in maximal acid output. • Liquid emptying is increased due to the loss of accomodation and receptive relaxation, with weakening of the duodenal brake. • Gastric emptying of solids are slowed due to motor paresis. • The vagus nerve usually suppresses ectopic pacemakers, which can disturb gastric emptying.
Parietal cell vagotomy: • 80-90% decrease in basal acid output and a 50-60% decrease in maximal acid output. • Gastric emptying of solids remain normal as the antrum and pylorus remain innervated. • Slight acceleration of liquid emptying due to loss of fundal reflexes.
Distal gastrectomy: • Removal of the antrum and pylorus leads to elimination of G-cells and loss of the synergism between gastrin and the vagus nerve. • Basal and maximum acid output are decreased by approximately 60%. • Solids of increasing particle size will empty quicker into the small bowel due to decreased resistance to outflow. • Gastric emptying of liquids is normal to rapid due to a decreased gastric reservoir combined with decreased accommodation with the loss of antralgastrin.
Total gastrectomy: • Complete loss of reservoir function, acid and pepsin secretion. • Truncal vagotomy usually accompanies total gastrectomy resulting in vagal denervation of the GIT.
Delayed gastric emptying: • Presentation: Nausea Intermittent vomiting Weight loss Postprandial vomiting Epigastric fullness Abdominal pain • Rule out mechanical causes of obstruction: • Barium radiography : Not reliable to evaluate gastric emptying of solids. • Upper gastrointestinal endoscopy: Document adequacy of the anastomosis. • Radionuclide scanning is useful to quantify the delayed emptying of solids and liquids through the gastric remnant and Roux limb.
In 1992 four types of partial obstruction were described by Gowen after Roux-en-Y gastrojejunostomy. • Type I and II were found immediately after surgery when feeding was introduced. • Type III and IV developed within 1-6 years of follow up. • In 1984 the etiology of gastric outlet obstruction due to anastomotic obstruction after Roux-en-Y gastrojejunostomy was explored.
Type I: • Kinked loop of jejunum 10-15cm below the anastomosis, where the jejunum passes through the transverse mesocolon.
Type I: • Upper gastrointestinal series were misinterpreted as an anastomotic obstruction. • Upper gastrointestinal endoscopy revealed a patent anastomosis, with 2-3cm narrowing of the jejunum 10-15cm distal to the anastomosis. • Endoscopic treatment: Manipulation of gastroscope in four directions at the anastomosis to loosen and stretch recently formed adhesions. • Endoscopic manipulation needed to be repeated in 2 of the 6 patients (33%), with no further surgical intervention needed in the 5 – 12 year follow-up period.
Type II: • Gastrojejunal anastomosis is too high on the gastric fundus creating a dependent sac that cannot empty by gravity.
Type II: • Upper gastrointestinal series revealed delayed gastric emptying with a high anastomosis. • Endoscopy confirmed a patent anastomosis but too high for effective drainage. • Surgical treatment: New side to end gastrojejunostomy in a more dependent position.
Type III: • Marginal ulcer
Approach to marginal ulceration: • Alkaline reflux • Anti-inflammatory drugs (stomach side) • Incomplete vagotomy • Incomplete gastrectomy • Retained antrum • Zollinger-Ellison syndrome • Malignancy
Type IV: • Gradual development of jejunal pouch due to three possible mechansims. • IV a: Development of an overhanging pouch gradually increasing in size, that will later fill preferentially from gastric fundus. As the pouch increases in size it may start to compromise the outflow tract.
IV b: Mesenteric wall of the jejunal segment tents upwards into the anastomosis with drainage of the stomach on both sides of the bar. Anatomic deformity develops similar to type IV a.
IV c: Postoperative adhesion formation between anastomosis and the liver or abdominal wall, angulating the anastomosis with pouch formation.
Anastomotic obstruction: • Gastric outlet obstruction after Roux-en-Y gastrojejunostomy. Van Marle J, Laage NJ, MaraisTJ and Mieny CJ. South African Journal of Surgery Vol 22: No 4 Nov/Dec 1984. • Identified causes of anastomotic narrowing: • Too short Roux-en-Y limb • Incomplete vagotomy • Anti-inflammatory drug abuse • Ischaemic fibrosis • End-to-end anastomosis
Anastomotic obstruction: • 1. Length of Roux-limb: • Recommended length of the Roux limb is between 45-60 cm. • If the distance between the jejunojejunostomy is less than 45cm bile reflux may still occur with ulceration leading to delayed gastric emptying. • Surgical treatment: Revision of gastrojejunostomy with revision of length of Roux limb to at least 45cm distal to gastrojejunostomy.
Anastomotic obstruction: • 2. Incomplete vagotomy: • Marginal ulceration. • 3. Anti-inflammatory drugs: • Remains an important cause of atrophic gastritis and marginal ulceration. • Surgical treatment: Revision of gastrojejunostomy.
Anastomotic obstruction: • 4. Ischaemic fibrosis: • Excessive mobilization of the ascending limb or devascularization of the greater and lesser curvature of the stomach. • 5. End-to-end anastomosis: • Predisposes to narrowing with a side-to-end anastomosis recommended.
Other mechanical causes of delayed gastric emptying: • Intussusception • Malrotation • Internal herniation
Roux-stasis syndrome: • In 1984 the term “Roux-syndrome” was coined to describe early and late symptoms of post-Roux-en-Y gastroparesis. • The Roux stasis syndrome may appear in the immediate post-operative period (acute: 20-30%) or later (30%). • It is believed that patients presenting with this syndrome refers to a subgroup of patients with unrecognized pre-existing motility disorders. • Preoperative radionuclide gastric emptying studies have so far been unsuccessful in predicting patients at high risk.
Pathophysiology of Roux-stasis: • Gastric remnant • Roux limb • The relative contributions to stasis are not entirely clear.
Gastric remnant: • Vagotomy decreases the tone of the gastric remnant and causes a motor paresis. • Reflux of biliary and pancreatic secretions (Billroth I and II) may facilitate gastric emptying from an atonic vagotomized gastric remnant by liquifying undigested food. • Roux-en-Y gastrojejunostomy prevents biliary reconstruction with dry and undigested food emptying from the gastric remnant.
Roux limb: • Disordered motility of the Roux limb is due to separation of the Roux limb from the duodenal pacemaker. • The duodenal pacemaker increases the frequency of jejunal contractions. • After transection the frequency distal to the cut decreases. • Ectopic pacemakers appear in the Roux limb.
Roux limb: • Ectopic pacemakers has a 25% reduction in frequency. • The pacemakers often appear downstream from the site of the transection with subsequent oral propagating electrical waves. • Small intestinal content driven in a proximal direction increases the resistance to outflow from the gastric remnant.
Alterations in gastrointestinal emptying of 99m-technetium labeled solids following sequential antrectomy, truncalvagotomy and Roux-Y gastroenterostomy.Vogel SB; Vair DB; Woodward ER. • Three patterns of delayed gastric emptying in dogs following a vagotomy and Roux limb reconstruction: • Poor emptying of solids out of the stomach. • Rapid emptying of solids out of the stomach, with regurgitation of material back into the stomach. • Roux limb stasis itself.
Medical Treatment: • Medical therapy for Roux stasis syndrome is seldom successful and revisional surgery is often required. • Nutritional support should focus on attempts to use enteral feedings by tube with the tip of the tube well beyond the stomach. • Metoclopramide has been the agent most widely used with variable success. • Other agents: Bethanechol, Domperidone and Cisapride.
Surgical Treatment: • If studies discriminate the stomach as the cause of the stasis more than the Roux limb, extensive gastric resection or completion gastrectomy are advocated. • Only a 1-3cm gastric rim is left of the proximal stomach to ensure a leakproof anastomosis. • Adjustment of the retrocolic Roux limb to a final length of 40cm.
Surgical Treatment: • Roux limbs longer than 50cm predisposes to stasis. • Persistence of Roux stasis syndrome is the major negative outcome. • No current method is available to reverse the motor abnormalities in the Roux limb once the limb has been constructed.
Rho-shaped Roux-en-Y gastrojejunostomy: • Postulate the presence of ectopic pacemaker at the top of the rho-shaped intestine, will allow flow in two directions preventing delayed gastric emptying. Motohiro et al World J of Surgery 2009 (33)
Rho-shaped Roux-en-Y gastrojejunostomy: Motohiro et al World J of Surgery 2009 (33)
Randomized Controlled Trial of Roux-en-Y Versus Rho-Shaped-Roux-en-Y Reconstruction (rRY) After Distal Gastrectomy for Gastric Cancer.Motohiro et al. World Journal of Surgery 2009(33). • rRY is a safe method but no advantage could be found above the usual RY reconstruction. • Extensive lymphnode dissection was not associated with delayed gastric emptying. • Truncal vagotomy was associated with inhibition of delayed gastric emptying.
Advantages and Disadvantages of Roux-en-Y Reconstruction after a Distal Gastrectomy for Gastric Cancer.Yoshiyuki et al. Surgery Today 2009 (39) 647-651. • Advantages: • Prevention of reflux oesophagitis • Prevention of gastritis and gastric cancer in residual stomach. • Reduced risk of suture rupture • Disadvantages: • Stomal ulcer • Roux stasis syndrome
Roux stasis syndrome: • Incidence of 30% • Uncut Roux-en-Y conserves duodenal pacemaker and prevent Roux stasis syndrome. • Length of Roux-en-Y limb is 30-35cm as the frequency of symptoms are higher when limb is > 40cm. • Food retention can be severe when large residual stomach is present. • Recommend: Not to leave a large section of the upper stomach as it is not needed for mixing or peristalsis. Yoshiyuki et al. Surgery Today 2009 (39)
In Japan Billroth I operation remains the first choice after a distal gastrectomy due to low incidence of anastomotic leakage and the shorter duration of surgery in comparison to Roux-en-Y. • Roux-en-Y can be used in high risk patients for anastomotic leakage (elderly, obese, DM, liver cirrhosis, chronic renal failure) and in esophageal hernia because of reduced duodenogastric reflux. Yoshiyuki et al. Surgery Today 2009 (39)
Long term follow-up of patients with Roux-en-Y Gastrojejunostomy for gastric disease.McAlhany JC et al. Annals of Surgery vol 219: 451-457. • Clinical condition that prompted surgery was corrected in 95%. • Roux-en-Y was successful in treating or preventing bile reflux gastritis in all cases. • Clinical failure (Visick scale III or IV) was documented in 8 patients (36%). • Roux stasis syndrome developed in 27% (6 of 8 patients).
Latest Results (12-21 years) of a Prospective Randomized Study Comparing Billroth II and Roux-en-Y Anastomosis after a Partial Gastrectomy Plus Vagotomy in Patients with Duodenal Ulcers. Csendes et al. Annals of Surgery Volume 249 (2), Feb 2009. • Compared clinical endoscopic and histological findings in patients. • Roux-en-Y gastrojejunostomy is significantly better than a Billroth II reconstruction.
Conclusion: • Incidence of Roux stasis syndrome: 20-30%. • Reserve for patients at high risk for anastomotic leakage, patients with concomittant oesophageal hernia and patients with dumping or biliary reflux after Billroth I and II. • Small gastric remnant • Roux limb: 30-40cm. • Uncut Roux-en-Y gastrojejunostomy • Always exclude mechanical causes.
Source: • Gastric atony and the Roux syndrome. Bruce David Schirmer. Gastroenterology Clinics of North America Volume 23 (2) June 1994. • Mayo Clinic Gastrointestinal Surgery. Kelly, Sarr and Hinder. • Preoperative and postoperative motility disorders of the stomach. Summers GE, Hocking MP. Surgical Clinics of North America. • Postgastrectomy syndromes. Eagon JC, Miedema BW, Kelly KA. Surgical Clinics of North America • Surgical options in postgastrectomy syndromes. Delcore R, Cheung LY. • Woodward’s Postgastrectomy Syndromes. Hocking and Vogel. • An alternative to Roux-en-Y for treatment of bile reflux gastritis. Van Stiegmann G, Goff JS. Suregry, Gynecology and Obstetrics Jan 1988 Volume 166.