Download
1 / 1
10 likes | 165 Vues
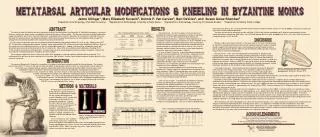
Jaime Ullinger 1 , Mary Elizabeth Kovacik 2 , Dennis P. Van Gerven 3 , Bert DeVries 4 , and Susan Guise Sheridan 2

E N D
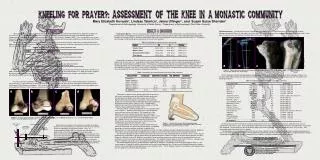
Jaime Ullinger1, Mary Elizabeth Kovacik2, Dennis P. Van Gerven3, Bert DeVries4, and Susan Guise Sheridan2 1Department of Anthropology, Ohio State University; 2Department of Anthropology, University of Notre Dame; 3Department of Anthropology, University of Colorado-Boulder; 4Department of History, Calvin College were eburnated, while 21.0% (11/53) of the monks demonstrated clear bone-on-bone contact (x2=13.6, p=0.0002). No right first metatarsals from Umm el-Jimal exhibited eburnation. The same proved true for osteophytic growth, with 29% (17/59) of the right first metatarsals at St. Stephen’s demonstrating at least “barely discernible” osteophytes, while only 1.3% (1/75) from Bab edh-Dhra’ (x2=20.9, p<0.0005) and 4.8% (1/21) from Umm el-Jimal had osteophytic growth (x2=5.8, p=0.02). Kneeling Facets: Results of metatarsal facet occurrence at Byzantine St. Stephen’s were compared to a variety of collections. Forty-six (10.1%) of the 453 scorable monastic metatarsals demonstrated kneeling facets. Ubelaker (1979) reported that an Ecuadorian (Ayalan) community had facets on 19.5% (106/544) of the metatarsals examined. Regional counterparts to the Byzantine St. Stephen’s collection showed lower frequencies, with Bab edh-Dhra' demonstrating 6.9% (30/430) and Umm el-Jimal at 7.8% (14/179). Markedly reduced numbers were found in several North American collections, both ancient and modern (Table 2). As seen in Table 3, there was a significant difference between the frequency of total kneeling facets for the monks, compared to all the North American collections, and the Ayalan group. However, no significant differences were found when compared to their regional counterparts at Bab edh-Dhra' and Umm el-Jimal. To avoid duplicating individuals, right metatarsals were selected for comparisons, as no significant side difference in kneeling facets was found for any of the collections (Table 4). There were no significant differences in facet frequency for the Byzantine St. Stephen’s right first metatarsals when compared to the other collections (Table 5). No kneeling facets were found in the first metatarsals from Umm el-Jimal. There were more facets on the third and fourth metatarsals for both Byzantine groups (St. Stephen’s and Umm el-Jimal) compared to Bab edh-Dhra’. Joint Surface Changes: The Byzantine St. Stephen’s collection showed considerably greater degenerative joint disease when compared to the Jordanian collections. Over half of the first metatarsals from Bab edh-Dhra’ and Umm el-Jimal had barely discernible lipping, while more than half from Byzantine St. Stephen’s had severe lipping with sharp ridge formation. Forty percent (11/27) of the monks’ first left metatarsals had surface porosity, compared to 12.0% for Bab edh-Dhra’ (x2=8.9, p=0.01). However, there was there was no difference between the monks and their Byzantine contemporaries at Umm el-Jimal (x2=2.8, p=0.2). There was a highly significant difference in eburnated right first metatarsals among the groups. Only 1% (1/74) from Bab edh-Dhra’ Table 1. Metatarsophalangeal joint surface changes The nature of lower limb activity has been extensively studied in skeletal remains from Byzantine St. Stephen’s monastery in Jerusalem. Previous studies have shown markers of repetitive kneeling on the bones of these monks. The hip, knee and ankle all exhibit modification suggesting repetitive activity consistent with daily prayer, as noted by ancient sources. Alterations of the foot were examined to flesh out the lower limb activity markers. As defined by Ubelaker (1979), these “kneeling” facets are found on all metatarsals (first through fifth), although they are primarily located on the second, third, and fourth metatarsals. For this monastic collection, there was no significant difference between right and left metatarsals (x2=0, p=1.0). Twenty-three of 227 (10.1%) total right metatarsals demonstrated “kneeling” facets; approximately 20% of the second and third metatarsals had them. Many of the metatarsals also exhibited osteoarthritis on the first metatarsophalangeal joint. Lipping, surface porosity, osteophytic growth and eburnation were examined on the distal joint of the first metatarsals. Many of the toes exhibited some modification, including 20.8% (11/53) of right first metatarsals with eburnation. The eburnation, porosity, and osteophytic growth occurred on the plantar surface of the foot, while the “kneeling” facets were located on the dorsal surface. These findings suggest that at least some of the monks were engaged in sustained, repetitive hyperdorsiflexion of the foot. This, combined with the presence of facets and imprints on the femur, tibia, and talus, lead to a better understanding of the daily postures of this monastic community. Previous studies have shown alterations in the lower limbs of the monks from Byzantine St. Stephen’s consistent with historical accounts of repetitive kneeling for prayer. Liturgical records suggest that the Byzantine monks may have been kneeling hundreds of times a day for prayer/genuflection (Bautch 1999; Driscoll and Sheridan 2000), possibly resulting in the presence of metatarsal modification. Kneeling Facets: Over 10% of all metatarsals from Byzantine St. Stephen’s had kneeling facets, which Ubelaker (1979:682) elsewhere attributed to “frequent, extreme hyperdorsiflexion of the metatarsophalangeal joints” (Figure 2). Among the prehistoric Native American groups cited, it was posited that these anatomical alterations resulted from habitually grinding corn. Molleson (2000:312) reported this pattern for the Neolithic people at Abu Hureyra, where osteophytic growth was found to be “remarkably exuberant” in older individuals, resulting from the “demands of grain preparation and grinding.” Joint Surface Changes: Osteoarthritis was more prevalent among the St. Stephen’s monks than for either regional counterpart. It was markedly stronger on the plantar vs. dorsal surface. A comparable pattern of arthritis of the first metatarsophalangeal joint accompanied by a kneeling facet was reported in Lovell and Dublenko (1999), and was Table 2. Metatarsal facet frequencies for each collection Figure 2. Relation of the metatarsals during kneeling & the extreme hyperdorsiflexion at the metatarso-phalangeal joint.Adapted from Ubelaker (1979). The monks of Byzantine St. Stephen’s, a monastery in Jerusalem, have been thoroughly studied for the past decade. The skeletal remains date from 5th-7th centuries AD and constitute one portion of a biocultural synthesis, which has reconstructed several aspects of the monks’ lives, including habitual, repetitive kneeling (Sheridan 1999, Driscoll and Sheridan 2000). Several studies have examined the nature of repetitive kneeling in the skeletal remains from St. Stephen’s, including the examination of musculoskeletal lesions (Hayden et al. 2004), non-metric features of the distal femur and proximal tibia (Kovacik et al. 2004), “squatting facets” (Ullinger et al. 2004) and morphological features of the femoral neck (Jennings et al. 2004). This study of the foot adds to the growing knowledge of lower limb activities in the Byzantine monks. The metatarsals from St. Stephen’s were compared to pedal bones from Umm el-Jimal, a contemporary non-monastic site in Jordan, and Early Bronze Age II-III (2850 – 2300 BC) remains from Bab edh-Dhra’, Jordan. Muehleman and Kuettner (2000:691) stated that the medial groove for the sesamoid is a frequent spot for cartilage degeneration, particularly as a result of dorsiflexion. Of interest to this study is their suggestion that “biomechanical imbalance rather than loading history” results in plantar surface damage of the metatarsal head. This may suggest that there was sublaxation of the sesamoid, as seen in modern clinical trails when sesamoiditis is aggravated by stair-climbing (Chou 2000). Previous studies of the St. Stephen’s calcanei also suggest movement along uneven terrain. Osteophytic growth is believed to be the result of repetitive stress and activity (Chou 2000). In clinical settings, it is referred to as hallux rigidus. The condition is typically present in older individuals, as it is degenerative (Kevin Pugh, personal communication). In a study of over 100 individuals opting for surgery to correct the condition, the average age of onset was 40 (Coughlin and Shurnas 2003). The overall average age of death for the St. Stephen’s community was mid-to-late 40s, however it was not possible to directly determine age from the metatarsals. Thus, it is possible that if there were significantly more older monks represented by the St. Stephen’s toes compared to the two Jordanian collections, this could explain the significantly higher frequency of osteoarthritis at the monastery. While kneeling facets were comparable across the three Near Eastern groups in this study, osteoarthritic changes were significantly more frequent in the metatarsophalangeal joints of the Byzantine monks. It is important to remember that these modifications were likely exacerbated by climbing and walking the hills of Jerusalem. Nevertheless, this study compliments the data gleaned from the hips, knees, and ankles of the monks, which when combined with the historical records, creates a strong circumstantial case that kneeling behavior took a considerable toll on the lower limbs of the members of this monastic community. Table 3. Comparison of metatarsal facets to St. Stephen’s Kneeling facets are located at the distal end of the superior metatarsal surface, and are described as “usually flat with sharply defined proximal borders” (Ubelaker 1979). Facets were examined on all right and left, first through fifth metatarsals. Figure 1 illustrates facets on two second left metatarsals. Of the 771 metatarsals (1st through 5th) from Byzantine St. Stephen’s, 453 specimens could be scored. For Umm el-Jimal, 179 of the 334 were scorable, and 430 of 715 could be used from the Bab edh-Dhra’ collection. The first metatarsals were studied in further detail. They were scored for the Table 4. Metatarsal facet comparisons by side for each collection Table 5. Comparison of right metatarsal facets to St. Stephen’s National Science Foundation Research Experiences for Undergraduates Institute for Scholarship in the Liberal Arts; University of Notre Dame L’École Biblique et Archéologique Française de Jérusalem Dr. Pam Stone & Chris Crain, Department of Anthropology, Western Michigan University Dr. Kevin Pugh, Department of Orthopaedics, Ohio State University presence of lipping, surface porosity, eburnation, and osteophytic growth on the metatarsophalangeal joint surface. All data were collected according to Buikstra and Ubelaker (1994). Table 1 describes the various stages of joint surface change scored for the present study. Byzantine St. Stephen’s Project Laboratory for Biocultural Studies Department of Anthropology University of Notre Dame Figure 1. Kneeling facets on the posterior end of second left metatarsals [EBND 11.13 & EBND 27.126]. associated with kneeling during canoe travel. The St. Stephen’s eburnation was not likely the result of hallux valgus (lateral deviation of the great toe), as Mays (2005) reported damage on both surfaces of the joint for this disorder.