Download
1 / 81
810 likes | 1.06k Vues
Smoking and Interstitial Lung Diseases Katerina M. Antoniou, MD, PhD ERS 1.05 Group Secretary Lecturer in Thoracic Medicine Medical School, University of Crete. Trieste, Italy, April 2013, ERS School , Pneumotrieste 2013.

E N D
Smoking and Interstitial Lung Diseases Katerina M. Antoniou, MD, PhD ERS 1.05 Group Secretary Lecturer in Thoracic Medicine Medical School, University of Crete Trieste, Italy, April 2013, ERS School , Pneumotrieste 2013
The direct pathogenetic relationship between cigarettesmoking respiratory diseases such as emphysema,(COPD), andlung cancer is well documented. • Regarding interstitiallung damage there is strong evidence providing links withcigarette smoking.
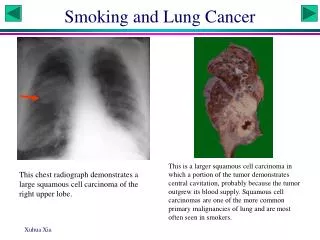
Introduction • Smoking triggers several diffuse lung diseases, including RB-ILD, DIP , LCH and perhaps IPF. • It is widely known that in asymptomatic smokers with normal lung function, chest radiography reveals the presence of interstitial opacities (dirty lung).
Introduction There are proven smoking-related processes that may fibrose – this is uncertain There are fibrotic disorders which may be driven by smoking – this is uncertain There is no proven smoking related pulmonary fibrosis
Referral pattern change:1995 2005 • Smoking-related diseases • NSIP / UIP • Sarcoid • Atypical TB / aspergillosis • Normal • Langerhans CH • Lymphangioleiomtis • Extrinsic Allergic Alveolitis • Usual interstitial pneumonia
Summary (1) • Interstitial lung abnormalities were present in 194/2416 (8%) of HRCTs • These abnormalities were associated with: • Reduced TLC (p<0.001) • Lower % of emphysema (p<0.001) • Restrictive lung deficit (TLC<80%) • Not met the diagnostic criteria for COPD
The pathobiology of smoking can lead to two distinct patterns of injury — emphysema (with destruction of the lung) or interstitial lung disease (with macrophage accumulation and fibrosis). • relative lack of emphysema could be simply • a reflection of the fact that the interstitial lung • abnormalities mask emphysema or that more • severe emphysema limits the extent of interstitial • lung abnormalities.
CLASSIFICATION OF IIP(IMMUNOCOMPETENT HOST) Idiopathic interstitial pneumonias (IIP) Idiopathic pulmonary fibrosis/Usual interstitial pneumonia (IPF/UIP) Lymphocytic interstitial pneumonia (LIP) Nonspecific interstitial pneumonia (NSIP) Cryptogenic organizing pneumonia (COP/OP) Respiratory bronchiolitis-associated interstitial lung disease (RBILD) Desquamative interstitial pneumonia (DIP) Acute interstitial pneumonia (AIP/DAD) 55% 25% 3% 15% 3% <1% Modified, ATS/ERS. Am J Respir Crit Care Med. 2002;165:277.
TABLE 1:Revised ATS/ERS Idiopathic Interstitial Pneumonia Classification: Multidisciplinary Diagnoses • Major Idiopathic Interstitial Pneumonias Idiopathic pulmonary fibrosis Idiopathic nonspecific interstitial pneumonia Respiratory bronchiolitis interstitial lung disease Desquamative interstitial pneumonia Cryptogenic organizing pneumonia Acute interstitial pneumonia • Rare Idiopathic Interstitial Pneumonias Idiopathic lymphoid interstitial pneumonia Idiopathic pleuropulmonary fibroelastosis • Unclassifiable idiopathic interstitial pneumonias† Travis DW, et al. AJRCCM 2013; in press
TABLE 2:CATEGORIZATION OF MAJOR IDIOPATHIC INTERSTITIAL PNEUMONIAS
Classification According to Disease Behavior • Reversible and self-limited (e.g. RBILD) • Reversible disease with risk of progression (e.g. cellular NSIP and some fibrotic NSIP, DIP, COP) • Stable with residual disease (e.g. some fibrotic NSIP) • Progressive, irreversible disease with potential for stabilization (e.g. some fibrotic NSIP) • Progressive, irreversible disease despite therapy(e.g. IPF, some fibrotic NSIP) Travis DW, et al. AJRCCM 2013; in press
Respiratory Bronchiolitis • RB represents ahighly specific physiological response to smoking. • RB ischaracterised by airway-centred accumulations ofmacrophages containing fine, granular yellowbrown cytoplasmic pigments (‘‘smoker’s macrophages’’)within distal bronchioles, alveolar ductsand adjacent alveolar spaces. • Cytoplasmic pigmentationis variable and correlates with the numbersof pack years smoked. Caminati A, et al. ERR 2012
Langerhans cell histiocytosis: an archetypal smoking-related disorder
Pulmonary Langerhans Cell Histiocytosis • “An uncommon destructive disorder of distal airways, caused by granulomas containing Langerhans cells.” • Macrophages are antigen processing or antigen presenting (dendritic)in type • The LC is a dendritic cell, derived from a bone marrow precursor and found exclusively in bronchiolar epithelium
Lung function tests can show eitherobstructive, restrictive or mixedabnormalities, even though theycan be normal in the early stage. • Reduced diffusing capacity of thelung for carbon monoxide (DL,CO)is present in a large proportion ofpatients. • In the treatment of PLCH, smokingcessation is a crucial step, as itleads to stabilisation of symptomsin the majority of cases.
Cigarette smoke: The recruitment and persistence of LCs in small airways arehighly likely to be the first pathogenic events in the diseaseprocess. Cigarette smoke may enable this through severalways.
Cigarette smoke: Alters the response of the airway mucosa to inhaled antigens,potentially amplifying the activation of dendritic and LCs toinfectious agents and allergens deposited in the airway. Cigarette smoke also promotes the survival of dendritic cellsby inducing cellular response proteins involved in the regulationof cell deathby apoptosis.
Cigarette smoke: 1. It is likely that accumulatingLCs around small airways lead to secondary recruitmentof other inflammatory cells and the formation of bronchiolocentric granulomatous-like lesions. 2. Inaddition, excessive generation of osteopontin in the lungmay promote macrophages and LC accumulation and persistence.
The persistent activation and retention of theseimmune cells may initiate a cascade of inflammatoryandfibrotic responses around the small airways that result inremodeling, deposition of scar tissue, and dilatation of structuresdistal to the small airways, eventually leading to cysticobstructed lesions of varying sizes.
RB-ILD DIP
Exaggerated form of smoking-related respiratory bronchiolitis • Generally benign/self limited vs survival • Significant symptoms/functional impairment
RB-ILD Patchy ground glass, bronchial wall and septal thickening
RBILD vs HPAsk the patient! BAL: lymphocytosis vs pigmented macrophages
NSIP versus DIPSmoking-related interstitial lung disease Hypothesis: A subgroup of cigarette smokers may develop a pattern of NSIP
AIM To explore possible links between smoking; and a) NSIP; b) IPF; c) rheumatoid lungand d) SSc-ILD
Does emphysema cluster with NSIP? Biopsy proven NSIP in smokers (n=18) Control cohort: Consecutive smokers in a smoking cessation clinic (n=137): Group A: COPD on GOLD criteria (n=34) Group B: Healthy smokers with normal FEV1 (n=103) HRCT evaluation
NSIP Findings Emphysema was present in 14/18 (77.8%) NSIP patients. Emphysema did not differ in prevalence between NSIP patients and control smokers with COPD (25/34, 73.5%) on univariate analysis and on multiple logistic regression. Emphysema was strikingly more prevalent in NSIP patients than in Group B control subjects (18/103, 17.5%), p<0.0005. Marten K, Milne D, Antoniou KM, et al. Eur Radiol. 2009
Our study addresses links between smoking and disease progression, as judged by severity-adjusted survival.
* * * identical severity-adjusted survival
Pathogenesis? Cottin V, et al. Thorax 2011 • The putative pathophysiology of SP-Cassociateddisease involves the dysfunctionof surfactant homeostasis. • Causes injury ordeath of alveolar epithelial type II cells andmyofibroblast proliferation.
Clinical Correlates: GERD Epithelial to mesenchymal transition Monocyte-derived cells: Fibrocytes Monocyte-derived cells: Alternatively activatedmacrophages Soluble mediators