HEMOCHROMATOSIS
230 likes | 1.12k Vues
HEMOCHROMATOSIS. Wendy Graham, MD, CCFP Academic ½ Day November 25, 2003. Pathophysiology. Inborn error in iron metabolism Increased iron absorption from the diet Iron overload Eventual fibrosis and organ failure Cirrhosis Cardiomyopathy Diabetes Hypogonadism.

HEMOCHROMATOSIS
E N D
Presentation Transcript
HEMOCHROMATOSIS Wendy Graham, MD, CCFP Academic ½ Day November 25, 2003
Pathophysiology • Inborn error in iron metabolism • Increased iron absorption from the diet • Iron overload • Eventual fibrosis and organ failure • Cirrhosis • Cardiomyopathy • Diabetes • Hypogonadism
Hereditary Hemochromatosis • Autosomal recessive disorder • Hemochromatosis gene (HFE) • Most common single gene disorder • 1/250 – 1/300 white persons is homozygous for the gene mutation • 1/10 carrier for mutation • 60-93% with disorder homozygous for the mutation C282Y (a cysteine–to-tyrosine substitution) • Also C282Y/H63D compound heterozygosity
Iron Overload • Net absorption of 3-4 mg/day • Accumulation of 500 to 1000 mg iron/yr • Clinical manifestations often occur after age 40 OR when stores are 15-40 g
Clinical Manifestations • Influenced by • Age • Sex • Dietary iron • Alcohol • Blood loss in menstruation and pregnancy • Unknown factors • Alcohol abuse and Hepatitis C accelerate • Classic description: cutaneous hyperpigmentation and diabetes in a patient with cirrhosis
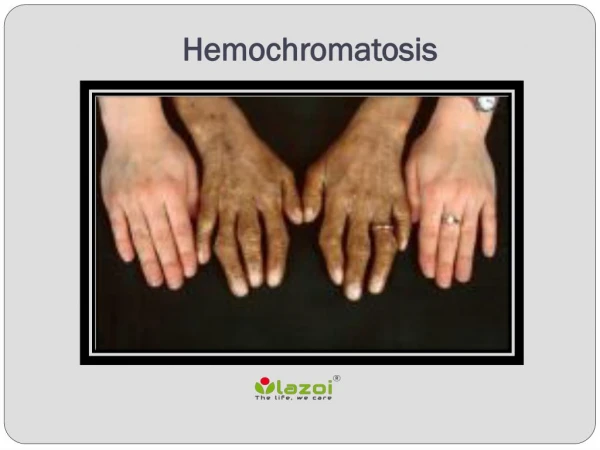
Reversible Manifestations • Heart: cardiomyopathy, conduction disturbances • Liver: abdominal pain, elevated LFTs, hepatomegaly (95%) • Skin: bronzing (melanin deposition), gray pigmentation (iron deposition) • Infection (Vibrio vulnificus, Listeria monocytogenes, Pasteurella pseudotuberculosis)
Irreversible Manisfestations • Liver: cirrhosis, hepatocellular carcinoma (most common cause of death) • Pituitary gland: gonadotropin insufficiency leading to secondary hypogonadism • Pancreas: diabetes mellitus (30-60%) • Thyroid: hypothyroidism • Genitalia: primary hypogonadism • Joints: arthropathy in MCPs (20-70%), pseudogout
Women & Hemochromatosis • Homozygosity is as common as in men • Symptomatic disease 10x less frequent • Presentation is later in women • Why? • Physiological blood loss in women and higher iron intake in men
Diagnosis • Combination of criteria • Clinical • Laboratory • Pathologic • Elevated serum transferrin saturation >45%(earliest abnormality) and an elevated serum ferritin • Caution serum ferritin = acute phase reactant • Confirmation = ‘gold standard” = liver biopsy (also defines extent of disease)
Treatment • Reserved for evidence of iron overload/complications • Desferrioxamine (DFO) ineffective • Avoid iron supplements, red meat • Avoid alcohol and tobacco • Avoid handling of raw seafood • Trestment = phlebotomy
Phlebotomy • Removal of 500 ml of blood • Removes 250 mg iron • Do weekly until iron depletion • Hgb < 120 • Ferritin < 50 • Transferritin saturation < 50% • 2-3 years may be required to remove >20g • Long term maintenance about once every 3 months
Genetic Testing • Gene on the short arm of chromosome 6 • Point mutations C282Y and H63D • HFE gene test in adult family members of an identified case • Should replace HLA typing • Pretest counselling (insurance, employment…) • Gene testing not recommended < 18 years • Done on whole bloold sample $200 U.S.
Screening • ?population screening • Looking @ WHO criteria likely cost effective • Not yet endorsed because need more information on disease burden and expression of disease • Ongoing study in Canada and U.S of 100 000 • Currently screen in patients who have: • Chronic liver disease • Signs and symptoms associated with the disease • A family history of iron overload



![[READ]⚡PDF✔ The Iron Disorders Institute Guide to Hemochromatosis: Symptoms, Relief, and Support for Hemochrom](https://cdn7.slideserve.com/12909563/the-iron-disorders-institute-guide-dt.jpg)