Download
1 / 22
220 likes | 283 Vues
Learn about hereditary hemochromatosis, a condition of excess iron absorption, common symptoms, genetic causes, and testing procedures to identify and manage the disorder effectively.

E N D
Hereditary Hemochromatosis Developed by Dr. Judith Allanson, Ms. Shawna Morrison and Dr. June Carroll Last updated April 2014
Disclaimer • This presentation is for educational purposes only and should not be used as a substitute for clinical judgement. GEC-KO aims to aid the practicing clinician by providing informed opinions regarding genetic services that have been developed in a rigorous and evidence-based manner. Physicians must use their own clinical judgement in addition to published articles and the information presented herein. GEC-KO assumes no responsibility or liability resulting from the use of information contained herein.
Objectives • Following this session the learner will be able to: • Refer to their local genetics centre and/or order genetic testing for hereditary hemochromatosis • Discuss and address patient concerns regarding family history of hereditary hemochromatosis • Find high quality genomics educational resources appropriate for primary care
Case • Michael is a 49-year-old male of Northern European descent with complaints of joint pain in his knees and hands. He is having a difficult time because his brother recently passed away at a young age. • Past Medical History: • Numerous office visits over 3–4 years for fatigue, weakness, and pain • Family History: • Michael is married with two healthy teenage sons (16, 14) • Father died at age 55 from myocardial infarction (MI) • Mother, 76, alive and well • Brother died at age 53 of esophageal varices • Sister, 55, has type II diabetes • Brother, 43, and sister, 40, alive and well CDC- NCBDDD http://www.cdc.gov/ncbddd/hemochromatosis/index.html
Family history 55 75 MI A&W d.53 55 49 43 40 Joint pain – knees and hand HPI fatigue, pain & weakness A&W Type II diabetes Esophageal varices A&W 14 16
Case • Social History: • Drinks "a couple of beers a week”, no tobacco or recreational drug use • No multivitamin use • Physical Exam: • Mild hepatomegaly • Modest enlargement of the second and third MCP joints
What is Hereditary Hemochromatosis? • Hereditary hemochromatosis is an inherited predisposition to absorb excess iron (Fe) from the diet • Mutations in the HFE gene are the most common cause of adult onset iron overload • In some predisposed individuals, excessive iron absorption and subsequent storage in various organs (i.e. liver, pancreas, heart, joints) eventually lead to cellular injury • If untreated, over time this can cause irreversible tissue/organ damage and shorten life expectancy • With early identification of at-risk individuals, surveillance of iron indices, and treatment when necessary, complications can be avoided
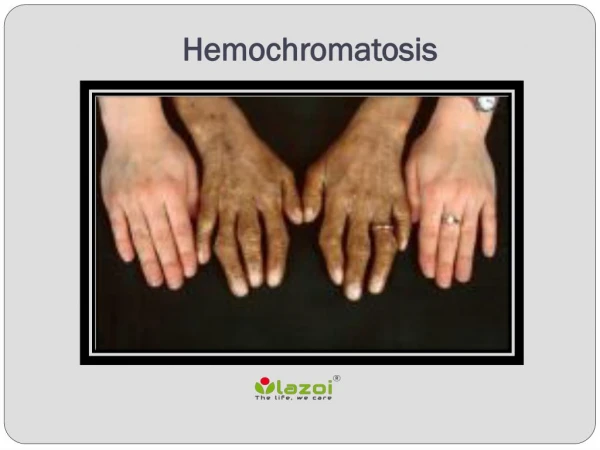
What is Hereditary Hemochromatosis? • Typically, symptoms of hereditary hemochromatosis present in men aged 40-60 and in post-menopausal women; however, onset is variable and can occur much earlier or much later. • Symptoms are nonspecific and include: • weakness, lethargy • skin discoloration (bronze or grey) • abdominal pain with or without hepatomegaly • joint pain and/or stiffness, arthritis • diabetes • cardiomyopathy • cirrhosis • hepatocellular carcinoma • testicular atrophy, erectile dysfunction • menstrual irregularity While any of these health concerns can be caused by hereditary hemochromatosis, the presence of two or more should greatly increase suspicion that the condition is present
What do I need to know about the genetics of Hereditary Hemochromatosis? • Autosomal recessive, with reduced penetrance • Caused by mutations in the HFE gene located on chromosome 6 • Standard testing by North American molecular genetics laboratories is targeted mutation analysis • Looks specifically for the two most common HFE mutations, C282Y and H63D • These account for over 90% of hereditary hemochromatosis • About 1 in 3 individuals of Northern European ancestry are carriers (heterozygotes) of the C282Y or H63D HFE gene mutations • About 1 in 260 individuals have two copies of (are homozygous for) the C282Y HFE gene mutation (genotype C282Y/C282Y)
Autosomal Recessive Inheritance Refresher C282Y carrier C282Y carrier C282Y / H C282Y / H H/ H C282Y/ H C282Y/ C282Y H / C282Y No HFE gene mutation C282Y carrier C282Y carrier Homozygous for C282Y ¼ - 25% ½ - 50% ¼ - 25% At risk for iron overload Actual risk depends on other genetic and non-genetic factors
Autosomal Recessive Inheritance Refresher Homozygous for C282Y No HFE mutation H / H C282Y / C282Y C282Y/ H C282Y/ H C282Y / H C282Y/ H 100% will be heterozygous for C282Y HFE mutation *can reveal non-paternity
Who should be offered biochemical testing for iron overload? • If your patient has suggestive symptoms, physical findings or a family history of Hereditary Hemochromatosis, transferrin saturation and serum ferritin are ideally ordered together to determine the likelihood of iron overload • Transferrin saturation (TS) • TS is a reliable screen for iron overload • Fasting TS of >45% is considered a sensitive but not specific threshold for identifying individuals who may have iron overload • Serum ferritin (SF) • In combination with persistent elevation of fasting TS, elevated ferritin is suspicious for iron overload • Rememberthat SF is an acute phase reactant that can be elevated by other inflammatory processes. Therefore an elevated SF does not necessarily imply iron overload and is not a reliable first or only screen
Who should be offered genetic testing? • Any adult with biochemical evidence of iron overload • >45% transferrin saturation (TS) and >300mg/L serum ferritin (SF) in men and post-menopausal women or >200mg/L SF in pre-menopausal women • Unexplained chronic liver disease and increased TS • An adult with a first-degree relative (sibling, parent or child) with one of the following genetic test results: • C282Y/C282Y (homozygote) • C282Y/H63D (compound heterozygote) • C282Y/S65C (compound heterozygote) • C282Y heterozygote (carrier) • Family history of iron overload, liver disease, type II diabetes, arthritis, heart disease (relatives with symptoms of HFE-hereditary hemochromatosis) Individuals with HFE-hereditary hemochromatosis occasionally demonstrate a normal TS and an elevated ferritin. If clinical suspicion is high and/or the patient has a positive family history, genetic testing is still warranted
What does the genetic test result mean? • The actual risk to develop iron overload is dependent on how many and which gene mutations have been inherited, in addition to other genetic and non-genetic factors • gender • alcohol intake • use of iron and vitamin C supplements • menstrual/pregnancy-associated iron losses
What does the genetic test result mean? • Two mutations identified in an individual with biochemical evidence of iron overload confirm Hereditary Hemochromatosis diagnosis • Two mutations identified in an asymptomatic individual suggest risk of developing iron overload and yearly monitoring of iron indices is recommended
How do I order the genetic test? • Genetic testing is performed on a blood sample • Will only assess risk to develop Hereditary Hemochromatosis or confirm diagnosis in symptomatic patient • It is important to include the following information on any requisition for the best test interpretation: • Indication for testing e.g. ‘symptoms of indicated disease’ or ‘abnormal iron indices’ or ‘positive family history’ • Ethnicity e.g. Northern European • Relevant family history e.g. parent/sibling with Hereditary Hemochromatosis (include genetic test results of affected individual if known) • Relevant medical history/investigations; e.g. biochemical iron overload
How will genetic testing help you and your patient? • If mutations are identified • Appropriate surveillance and management of risk of iron overload • If no mutations are identified • If your patient was tested because of a known family mutation, he/she no longer needs frequent monitoring of iron indices and is not at increased risk to develop iron overload. The test has ruled out Hereditary Hemochromatosis • If your patient was tested because of a reported positive family history, more information is needed before ruling out HH in this individual. Your patient should be encouraged to obtain confirmation of the familial mutations and/or diagnosis • If your patient was tested because of persistently high iron indices, additional investigations should be considered
Are there harms or limitations of genetic testing? • Potential harms • Insurance discrimination • Genetic testing in an asymptomatic individual may affect his/her ability to obtain life, disability, critical illness, long-term care and/or extended health insurance • Hereditary Hemochromatosis is a treatable condition and some insurance companies will not deny coverage to a treated individual • Non-paternity could be revealed • Limitation • Targeted mutation analysis • Not every HFE gene mutation is looked for, however, the most common mutations account for more than 90% of all mutations, thus fewer than 10% will be missed using current testing strategies
Case • Blood work demonstrates biochemical evidence of iron overload • Ferritin >300mg/L AND TS >45% • + suggestive family history [MI, liver disease with iron overload, type II diabetes in first degree relatives] • You suspect Hereditary Hemochromatosis and offer genetic testing • Michael accepts and the result shows he is homozygous for C282Y HFE gene mutation
Surveillance and management • Patient identified to have two HFE gene mutations* • Annual monitoring of serum ferritin (SF) • Normal • Increased • Continue annual SF monitoring • Refer to specialist (e.g. gastroenterologist, hematologist)
Pearls • Hereditary Hemochromatosis is a common inherited predisposition to absorb excess iron from the diet caused by mutations in the HFE gene • Most individuals with the predisposition do not develop clinical disease • Hereditary Hemochromatosis has the potential to cause morbidity and mortality. With early identification of at-risk individuals, appropriate surveillance of iron indices, and treatment when indicated, complications can be avoided • Genetic testing should be considered for: • Adults with biochemical evidence of iron overload (>45% fasting transferrin saturation and >300mg/L serum ferritin in men and post-menopausal women or >200mg/L SF in pre-menopausal women) • Any adult whose first-degree relative has the C282Y HFE gene mutation • Individuals with suggestive family histories
References • Bacon BR, Adams PC, Kowdley KV, Powell LW, Tavill AS, American Association for the Study of Liver Diseases. Diagnosis and management of hemochromatosis: 2011 practice guideline by the American Association for the Study of Liver Diseases. Hepatology 2011; 54: 328–43 • European Association for the Study of the Liver. EASL clinical practice guidelines for HFE hemochromatosis. J Hepatol 2010; 53:3–22. • Kowdley KV, Bennett RL, Motulsky AG. HFE-Associated Hereditary Hemochromatosis. 2000 Apr 3 [Updated 2012 Apr 19]. In: Pagon RA, Adam MP, Bird TD, et al., editors. GeneReviews™ [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2014. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1440/ • Wallace DF, Walker AP, Pietrangelo A, Clare M, Bomford AB, Dixon JL, Powell LW, Subramaniam VN, Dooley JS. Frequency of the S65C mutation of HFE and iron overload in 309 subjects heterozygous for C282Y. J Hepatol 2002; 36(4):474-9. • Centre for disease Control and Prevention. National Center on Birth Defects and Developmental Disabilities. Hemochromatosis. http://www.cdc.gov/ncbddd/hemochromatosis/index.html [Accessed September 2013]