Download
1 / 111
1.34k likes | 3.39k Vues
Non-neoplastic diseases of oral cavity. Dr. Vishal Sharma. Common diseases. Sub-mucous fibrosis Aphthous ulcer Leukoplakia Erythroplakia Oral candidiasis Oro-labial Herpes Vincent’s infection Infectious mononucleosis Tongue tie Geographic tongue

E N D
Non-neoplastic diseases of oral cavity Dr. Vishal Sharma
Common diseases Sub-mucous fibrosis Aphthous ulcer Leukoplakia Erythroplakia Oral candidiasis Oro-labial Herpes Vincent’s infection Infectious mononucleosis Tongue tie Geographic tongue Ranula Mucocoele
Oral pre-malignant conditions • Oral sub-mucous fibrosis • Leukoplakia & Erythroplakia • Oral candidiasis • Lichen planus • Nicotinic stomatitis (smoker’s palate) • Tertiary syphilis • Mucosal hyper-pigmentation (melanosis)
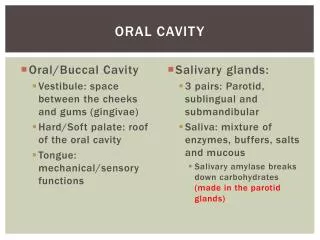
Infection:Herpes, Vincent’s infection, Candidiasis • Auto-immune:Aphthous ulcer, Behcet’s syndrome • Trauma:cheek bite, jagged tooth, ill-fitting denture chemical burn, thermal burn • Skin disorder:Lichen planus, erythema multiforme • Blood disorder:Leukemia, agranulocytosis, pancytopenia, sickle cell anemia • Drug allergy:mouth wash, toothpaste • Neoplasm: benign, malignant • Others:Radiation, chemotherapy, diabetes, uremia
Definition • Term coined byS.G. Joshiin 1953 • Chronic pre-malignant disease of oral cavity, characterized by juxta-epithelial inflammation + progressive fibrosis of lamina propria & deeper connective tissues, followed by stiffening of mucosa resulting in difficulty in mouth opening
Etiology (multi-factorial) 1.Areca nut (betel nut) chewing 2.Tobacco & Paan masala chewing 3.Genetic predisposition 4.Auto-immune injury 5.Nutritional deficiency of vitamins, iron, anti-oxidants 6.Excessive alcohol consumption 7.Excessive consumption of chilies (controversial)
Presenting symptoms • Burning pain on consumption of spicy food • Dryness of mouth • Impaired mouth movements while eating & talking • Progressive inability to open the mouth (trismus) • Hearing loss (stenosis of Eustachian tubes) • Nasal intonation (ed soft palate mobility)
Clinical Staging Stage of stomatitis:red mucosa vesicles rupture to form mucosal ulcers Stage of fibrosis (healing):blanching of mucosa, fibrous bands in oral mucosa, trismus, ed soft palate mobility Stage of sequelae:difficult speech, hearing loss, leukoplakia, malignancy (3 - 8 %)
Medical Treatment 1. Bi-weekly submucosal intra-lesional injections ofDexamethasone4 mg +Hyaluronidase1500 IU for 6- 8 wks 2. Submucosal injection of human placental extract 3. Vitamin B complex + anti-oxidant supplement 4. Avoid consumption of mucosal irritants 5. Increased intake of fruits & vegetables
Surgical treatment for trismus 1. Simple release of fibrous bands + skin grafting 2. Laser-assisted release of fibrous bands 3. Excision of lesions & reconstruction with: buccal fat pad, naso-labial flap, lingual flap, palatal muco-periosteal flap, radial forearm flap 4. Temporalis muscle myotomy + mandibular coronoidectomy
Introduction Recurrent, superficial ulcers, with necrotic centre + red margin, involving movable mucosa of inner surface of lips, cheeks, tongue & soft palate Differences from viral ulcer 1. Frequent recurrence 2. Selective involvement of movable mucosa 3. Absence of fever, malaise, lymph node enlargement
Types 1. Minor aphthous ulcer:2 – 10 mm in size, multiple, heal with no scar in 1 - 2 weeks 2. Major aphthous ulcer:20 – 40 mm in size, usually single, heal with scar over months 3. Herpetiform aphthous ulcer:< 1 mm in size, multiple, heal with no scar in 1 week
Major aphthous ulcer Rule out HIV & malignancy
Trigger factors for auto-immune injury Deficiency:vitamin B complex, iron, folic acid, zinc Stress:emotional & physical Trauma:cheek bite, ill-fitting dentures Hormonal imbalance:changing progesterone level Allergy:sodium lauryl sulphate (mouth wash & paste) Drugs:NSAIDs, cancer chemotherapy Others:Behcet’s syndrome, HIV, Crohn’s disease Infection:controversial
1. Avoid trigger factors 2. Supplement:vitamin B complex + folic acid + iron 3. Topical gel combination:ZYTEE, QUADRAJELa. steroid:triamcinolone b. antibiotic:chlorhexidine, metronidazole, benzalkonium, cetalkonium, tannic acid c. analgesic:benzydamine, choline salicylate d. anesthetic:lignocaine, benzocaine 4. Mouth rinse:betamethasone, tetracycline 5. Immuno-modulator:thalidomide 50 -100 mg daily
Behcet’s syndrome • Uveitis + Aphthous ulcer + Genital ulcer • Oculo – Oro - Genital syndrome • Tx:steroid
Introduction Definition:pre-malignant condition with white patch or plaque that cannot be rubbed off with gauze swab & cannot be characterized clinically or pathologically as any other disease Malignant transformation:1 - 20%(average 5 %) Sites:Buccal mucosa, tongue, lips, palate, floor of mouth, gingiva, alveolar mucosa
Etiology • Chronic smoking • Chronic tobacco chewing • Irritation from jagged teeth or ill-fitting dentures • Chronic alcohol consumption • Sun exposure to lips • Associated: submucous fibrosis, hyperplastic candidiasis, Plummer-Vinson syndrome, AIDS
Types of leukoplakia 1. Homogeneous leukoplakia:smooth, white 2. Nodular leukoplakia:nodular, white 3. Verrucous leukoplakia:warty, white 4. Speckled (erythro) leukoplakia:white + red Malignant potential: speckled >> nodular & verrucous >> homogenous
Pathological stages • Hyperkeratosis:thickening of stratum corneum • Parakeratosis:keratinization with retention of nuclei in stratum corneum(homogeneous leukoplakia) • Acanthosis:thickening of stratum spinosum(verrucous & nodular leukoplakia) • Dyskeratosis:abnormal keratinization present below stratum granulosum(speckled leukoplakia)
Investigations 1. Supra-vital staining / Ora-screen:Toluidine blue solution stains areas of malignancy 2. Biopsy:to rule out malignancy
D/D of oral white lesions • Leukoplakia • Hyperkeratosis • Hypertrophic candidiasis • Hairy leukoplakia (Epstein-Barr virus infection) • Lichen planus • Oral sub-mucous fibrosis • Lupus erythematosus • White sponge nevus • Carcinoma
Treatment 1. Removal of causative agent 2. Supplement:Vitamin A (beta-carotene), C, E, B12, folic acid 3. Surgical excision:if HPE showsdysplasia Surgical excision modalities:cold knife, cryosurgery, laser surgery
Cold knife excision AFTER BEFORE
Laser excision AFTER BEFORE
Definition:pre-malignant condition with red patch or plaque that cannot be rubbed off with gauze swab & cannot be characterized clinically or pathologically as any other disease Red colour due to vascular submucosal tissue shining through under-keratinized mucosa Malignant potential:17 times > leukoplakia Tx:excision biopsy
Etiology:Infection with Candida albicans Predisposing factors: 1. Chronic ill-health 2. Uncontrolled diabetes mellitus 3. Acquired immune deficiency syndrome 4. Prolonged use of steroids 5. Prolonged antibiotic therapy 6. Immuno-suppressant therapy (cyclosporine) 7. Anti-cancer chemotherapy
Types of oral candidiasis • Chronic hyperplastic:white plaques, cannot be removed by scraping(Candidal leukoplakia) • Pseudo-membranous:loosely adherent white lesions, can be scraped off leaving red patches • Erythematous (atrophic):smooth, red patches • Cheilitis:white lesions on angle of mouth