ORAL CAVITY
ORAL CAVITY. Clerk Sarah Camille Concepcion. OUTLINE. INTRODUCTION EMBRYOLOGY ANATOMY PHYSIOLOGY DISEASES. ORAL CAVITY. BOUNDARY : Vermilion border of the lips to junction of hard and soft palate and circumvallate papillae (tongue) . EMBRYOLOGY. Derived from the embryonic foregut


ORAL CAVITY
E N D
Presentation Transcript
ORAL CAVITY Clerk Sarah Camille Concepcion
OUTLINE • INTRODUCTION • EMBRYOLOGY • ANATOMY • PHYSIOLOGY • DISEASES
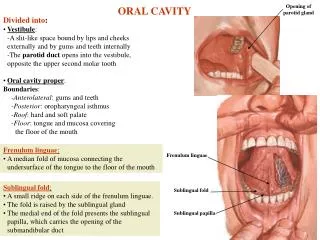
ORAL CAVITY BOUNDARY: Vermilion border of the lips to junction of hard and soft palate and circumvallate papillae (tongue)
EMBRYOLOGY • Derived from the embryonic foregut • Stomoduem • Primitive mouth that forms the topographic center of the developing face • Fusion of ectoderm & endoderm
EMBRYOLOGY OF ORAL CAVITY UPPER LIP • Fusion of medial frontonasal and lateral maxillary prominences • 6th-8th week of fetal devt LOWER LIP • Fusion of mandibular prominences • 4th week of fetal devt
EMBRYOLOGY OF ORAL CAVITY CHEEK • Formed by the buccinator muscle SALIVARY GLANDS • Develop from stomadeal ectoderm by ingrowth of oral epithelium into underlying mesenchyme • Starts at a 6 weeks AOG
EMBRYOLOGY OF ORAL CAVITY TONGUE • from lingual swellings and tuberculumimpar • ~4 weeks AOG PALATE • Fusion of primary and secondary plates • 12th week AOG MANDIBLE • Membranous ossification of Meckel’s cartilage • 4 ½ weeks AOG
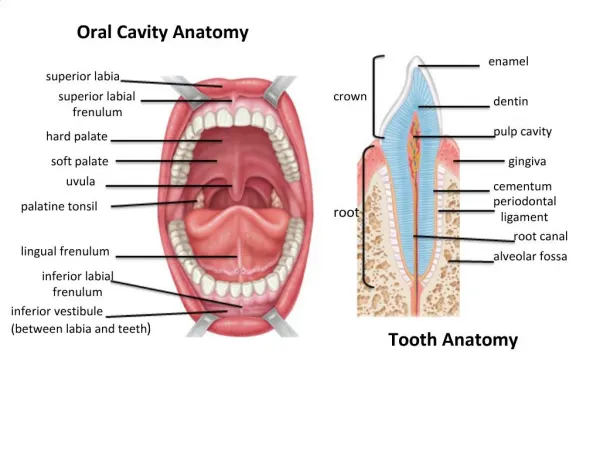
PARTS/SUB-UNITS • Lips • Buccal mucosa • Alveolar ridges • Anterior 2/3 of the tongue • Retromolartrigone • Floor of the mouth • Hard palate
LIPS & CHEEK • Vermillion • Red due to thin squamous epithelium • Vestibule • Region between internal mucosa of cheek and teeth • Orbicularisoris • Foundation of lips and cheeks
LIPS & CHEEK • Labial commissure • Nasolabial fold • Lips • Supplied by superior and inferior labial arteries • Drained by facial vein • Innervated by infraorbital (upper lip) and mental (lower lip) nerve
LIPS & CHEEK • Cheeks • Muscular framework formed by buccinator • Bichat fat pad (buccal fat pad) • Innervated by branches of the facial nerve
MUSCLES OF MASTICAITON • Masseter muscle • Temporalis muscle • Medial and lateral pterygoid muscles • Supplied by mandibular nerve (third division of the trigeminal nerve)
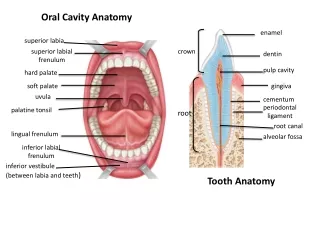
TEETH Infants: 2 I, 1 C, 2M Adults: 2 I, 1C, 2PM, 3M
Alveolar Ridge • thickened ridge of bone that contains the tooth sockets on bones that bear teeth • RetromolarTrigone • Area between the upper and lower posterior molars
SURFACE ANATOMY • Divisions: apex, body, and base • Terminal sulcus • Papillae • Filiform, fungiform, foliate, vallate • Foramen cecum • Frenulum lingua
Extrinsic muscles (CNXII) STYLOGLOSSUS GENIO- GLOSSUS HYOGLOSSUS GENIOHYOID MYLOHYOID
Intrinsic muscles (CNXII) A) VERTICAL M. - FIBERS SUP & INF - FLATTEN & BROADEN TONGUE CORONAL SECTION C) LONGITUDINAL M. - FIBERS ANT-POST. - SHORTEN TONGUE B) TRANSVERSE M. - FIBERS HORIZONTAL - NARROW TONGUE
TONGUE • Vascular supply: Lingual artery and vein • Motor innervation: CN XII • Sensory innervation: • Anterior 2/3 – lingual nerve chorda tympani • Posterior 1/3 – CN IX • Lymphatic drainage • ipsilateral and contralateralsubmandibular and submental lymph nodes
PALATE HARD PALATE • formed by palatine processes of the maxilla anteriorly, incisive bone, and horizontal plates of palatine bones posteriorly SOFT PALATE • Seals the oral cavity posteriorly • tensor velipalatini, levatorvelipalatini, palatoglossus, palatopharyngeus muscle
Vascular supply • ascending palatine branch of the facial artery Sensory innervation • greater and lesser palatine nerves from V2
PHYSIOLOGY • Importance for food intake • Mastication (teeth, tongue) • Digestion (salivary enzymes) • Taste (Gustatory, chemoreception) • Swallowing (Hard and soft palate) • Speech (phonation and articulation) • Tongue, cheeks, lips
SALIVA 1500 mL/day; pH 6.2-7.4 • 99.5% water • 0.5% organic/inorganic solids. • Na – 10 mEq/L • K – 26 mEq/L • Cl – 10 mEq/L • HCO3 – 30 mEqlL • glycoprotein and amylase
ORAL TORI - nodular or bony growth • Torus Palatinus • in the midline of hard palate • Torus Mandibularis • In the lingual aspect of the mandible TX: Surgery
MICROGNATHIA • Congenital or acquired diminution in size of the mandible • Failure at the growth center of the condyle • May be due to trauma • Some associated with syndromes TX: Surgery
ROBIN ANOMALY • Triad: • Cleft palate + Micrognathia + Glossoptosis • Symmetric lack of mandibuilar growth prevents adequate support of lingual musculature, allowing the tongue to fall downward and backward TX: mild case – keep the infant in prone position, suspend head by stocking cap severe – tongue tip sutured to anterior mandible or lower lip
PROGNATHISM • Enlargement or anterior placement of lower jaw TX: Surgery
MALOCCLUSION • Disturbed development of face and jaws • Underdevelopment of maxilla or mandible or overdevelopment of mandible
MACROGLOSSIA • Enlarged tongue that may result in abnormal speech • Due to increase in amount of tissue • Most are due to lymphangioma or hemangiolymphoma
MEDIAN RHOMBOID GLOSSITIS • Smooth to nodular, elevated or depressed area of void papillae • No treatment required
LINGUAL THYROID • Partial or complete embryologic failure of the thyroid gland to descend from the foramen cecum • No tx for small lesions • Before surgery, make certain that it is not the only throid tissue in the body
ANKYLOGLOSSIA • Inability to elevate the tongue tip above a line extending through the commissures of a congenitally short lingual frenulum • TX: frenulum clipped during infancy in severe forms
CLEFT LIP AND PALATE Unilateral incomplete Unilateral complete Bilateral complete
CLEFT LIP AND PALATE • Developmental anomaly of the embryonic head • Genetic inheritance • External influences: viral infections, placental oxygen deficiency, intrauterine bleeding, exposure to ionizing radiation • Symptoms: • Hypernasal speech (due to incomplete closure of the nasopharynx) • Recurrent middle ear effusions and inflammation resulting from eustachian tube dysfunction • Variable abnormalities of the nasal septum or in the shape of the external nose
CLEFT LIP AND PALATE • Diagnosis: palpation of the hard palate to detect bony discontinuity • Goals of surgery • To achieve closure of the hard and soft palate. • To provide soft palate sufficient length and mobility. • Treatment: lip/velum/palate repair, rhinoplasty, speech promotion/therapy • RULE OF 10 • 10 weeks, 10 pounds,10 g Hemoglobin
WHITE LESIONS OF THE ORAL MUCOSA • A change in color of the normally reddish oral mucosa to white. • One of the most frequently encountered oral abnormalities. • Leukoplakia-”white patch” that does not rub away • Frequently caused by increased retention and production of keratin by mucosal stratified squamous epithelium. • Biopsy may demonstrate cytologic alterations and may warrant consideration as “premalignant”
LICHEN PLANUS • present as fine lacework of white reticular keratoticpaules (wickham’sstriae) and gray plaque like or annular lesions on the dorsum of the tongue • On the buccal mucosa, the lesions originate in the posterior area and spread anteriorly. • Generally asymptomatic although a metallic taste or mild discomfort is common. • Superficial erosions, bullous lesions, and deep, chronic, painful, ulcerations occasionally occur.
Viral infections: Herpes simplex virus • Etiology: HSV type 1 (cutaneous and oral-mucosa strain) • Transmission: contact or droplet infection • Primary infection • Usually acquired in early childhood • Predominantly affects the oral mucosa as herpetic gingivostomatitis (aphthousstomatitis) • Appearance of local lesions (bullae) on the oral mucosa, preceded by fever and lethargy consistent with a flulike infection, accompanied by regional lymphadenitis
Viral infections: Herpes simplex virus • Reactivation of HSV • Occurs in response to physical exertion, UV radiation, febrile infection, emotional stress, pregnancy • Commonly manifested as herpes labialis • Site of predilection is perioral region, especially the mucocutaneous junction of the lips
Viral infections: Herpes simplex virus • Diagnosis: history & PE, classic giant cells by Tzanck smear • Complications • Herpes impetiginatus - secondary bacterial superinfection by S. aureus or streptococci • Postherpeticexudativeerythemamultiforme – skin lesions & typical ulcerative eruptions on the mucous membranes of the mouth, lips, and genitals • Treatment: topical antiseptics to prevent superinfection; acyclovir; 5-7days
Viral infections: Varicella-Zoster Virus • Chicken pox • Predominantly in children • VZV Primary infection • Symptoms • skin rash consisting of erythematous papules and thin-walled vesicles with watery contents, covering the body but especially pronounced on the head and trunk
Viral infections: Varicella-Zoster Virus • aphtha-like vesicles appear on the oral mucosa especially on the hard palate, buccal mucosa and gingiva • After the cutaneous lesions have healed, the virus persists in the ganglion cells of sensory nerves