Download

1 / 61
650 likes | 1.37k Vues
ACUTE RESPIRATORY DISTRESS SYNDROME. BY DR PRASHANT KINI . WHAT IS RESPIRATORY FAILURE?. IT IS A FAILURE OF THE PROCESS OF DELIVERING OXYGEN TO THE TISSUES AND REMOVING CO2 FROM THE TISSUES.

E N D
ACUTE RESPIRATORY DISTRESS SYNDROME BY DR PRASHANT KINI
WHAT IS RESPIRATORY FAILURE? • IT IS A FAILURE OF THE PROCESS OF DELIVERING OXYGEN TO THE TISSUES AND REMOVING CO2 FROM THE TISSUES. • IT OCCURS WHEN DYSFUNCTION OF THE RESPIRATORY SYSTEM RESULTS IN ABNORMAL GAS EXCHANGE THAT IS POTENTIALLY LIFE THREATENING.
TYPES HYPOXIC HYPERCAPNIC PACO2>45-55 MM HG PH<7.35 • PAO2<60 MM HG • SPO2<90 %
CONDITIONS CAUSING HYPOXIC HYPERCAPNIC MYASTHENIA GRAVIS ASCENDING POLYRADICULOPATHY MYOPATHIES ASTHMA COPD • SEVERE PNEUMONIA • PULMONARY OEDEMA • PULMONARY HAEMMORHAGE • ARDS
ARDS • ARDS IS A HYPOXIC RESPIRATORY FAILURE CAUSED BY ACUTE LUNG INJURY.
AMERICAN-EUROPEAN CONSENSUS CONFERENCE DEFINITION • ACUTE B/L PULMONARY INFILTRATES • RATIO OF PAO2 TO INSPIRED OXYGEN CONCENTRATION (FI02)<200 • NO EVIDENCE FOR HEART FAILURE OR VOLUME OVERLOAD AS THE PRINCIPAL CAUSE OF THE PULMONARY INFILTRATES.
FIRST DESCRIBED IN WORLD WAR II BY MILITARY PHYSICIANS. • OFFICIALLY NAMED IN 1960 S AFTER MECHANICAL VENTILATION WAS USED FOR PTS WITH RESPIRATORY FAILURE. • A INITIALLY STOOD FOR ADULT BUT LATER AS IT OCCURRED IN ALL AGE GROUPS IT WAS NAMED ACUTE.
OTHER NAMES • STIFF LUNG • WET LUNGS • SHOCK LUNG SYNDROME.
BASIC PATHOLOGY • INCREASED PERMEABILITY OF ALVEOLAR- CAPILLARY MEMBRANE. • DIFFUSE ALVEOLAR DAMAGE. • ACCUMALATION OF PROTEINACIOUS PULMONARY OEDEMA.
OLD CRITERIA • ORIGINALLY THERE WERE THREE CRITERIA • SEVERE HYPOXEMIA • DECREASED PULMONARY COMPLIANCE • DIFFUSE PULMONARY INFILTRATES ON CHEST RADIOGRAPH.
REVISED CRITERIA • ACUTE LUNG INJURY(MILD FORM OF ARDS) • PAO2/FIO2<300 MMHG (REGARDLESS OF PEEP LEVEL) • B/L INFILTRATES SEEN ON CHEST RADIOGRAPH • PULM ARTERY OCCLUSION PRESSURE < 18 MM HG WHEN MEASURED.
REVISED CRITERIA • ARDS • PAO2/FIO2 < 200 MM HG (REGARDLESS OF PEEP) • B/L INFILTRATES SEEN ON CHEST RADIOGRAPH. • PULM ARTERY OCCLUSION PRESSURE < 18 MM HG WHEN MEASURED.
MOST COMMON AT RISK CONDITIONS • SEVERE SEPSIS • MAJOR TRAUMA • ASPIRATION OF GASTRIC CONTENTS
OTHER RISK FACTORS • CHRONIC ALCOHOL ABUSE • CRITICALLY ILL PTS. • DIFFUSE PULM INFECTION • NEAR DROWNING • PULM CONTUSION • TOXIC INHALATION • HYPERTRANSFUSION • PANCREATITIS • CARDIOPULM BY PASS.
EARLY DIAGNOSIS • HIGH RESPIRATORY RATE • DYSPNOEA.
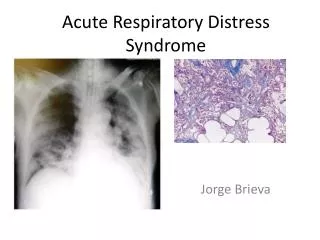
THROUGH INVESTIGATIONS • ARTERIAL BLOOD GASES • CHEST X RAY MAY BE CLEAR INITIALLY. • LATER MAY SHOW B/L PULM INFILTRATES.
PATHOPHYSIOLOGY • THREE PHASES • INITIATION • AMPLIFICATION • INJURY
INITIATION • PRECIPITATING EVENT • RELEASE OF CELLS AND IMMUNE MEDIATORS(TNF ALPHA , INTER;EUKIN 1)
AMPLIFICATION • RECRUITMENT, ACTIVATION OF NEUTROPHILS IN SPECIFIC TARGET ORGANS. • STIMULATION OF NEUTROPHILS BY INTERLEUKIN-8. • RELEASE OF REACTIVE OXYGEN METABOLITES AND PROTEASES.
INJURY • CELLULAR DAMAGE. • INJURY TO TYPE 2 PNEMOCYTES LEADING TO REDUCTION OF SURFACTANT SYNTHESIS.
AGGRAVATING FACTORS • INCREASED IV FLUID ADMINISTRATION • MYOCARDIAL DEPRESSION.
OTHER PATHOLOGICAL FEATURES • INCREASED AIRWAY RESISTANCE • BRONCHIAL WALL OEDEMA • ALVEOLAR COLLAPSE DUE TO FLUID ACCUMALATION. • PULMONARY VASOCONSTRICTION • INCREASED PULM VASCULAR RESISTANCE.
OTHER PATHOLOGICAL FEATURES • DENUDED BASEMENT MEMBRANE • WIDENING OF INTERCELLULAR JUNCTIONS • FORMATION OF HYALINE MEMBRANE • THROMBOSIS OF ALVEOLAR CAPPILARIES AND SMALL PULM ARTERIES.
PROGNOSIS • MORTALITY RATES HIGHER IN • OLD PTS • SEVERE SEPSIS • MULTIPLE ORGAN DYSFUNCTION
CAUSE OF DEATH • EARLY(WITHIN 72 HRS) • LATE(AFTER 3 DAYS)
EARLY • ORIGINAL PRESENTING ILLNESS • INJURY
LATE • SECONDARY INFECTION • PERSISTENT RESP FAILURE • MOD(MULTIPLE ORGAN DYSFUNCTION)
PROGNOSIS • IN SURVIVORS,PTS WILL CONTINUE TO HAVE RESTRICTIVE IMPAIMENT OR DECREASED DIFFUSING CAPACITY. • THOSE HAVING SEVERE ARDS WIL HAVE MORE PULM DYSFUNCTION COMPARED TO THOSE WITH MILD ARDS.
TREATMENT • MECHANICAL VENTILATORY SUPPORT • INTRAVASCULAR FLUID MANAGEMENT • PHARMACOLOGICAL THERAPY.
MECHANICAL VENTILATORY SUPPORT • AIM IS TO ACHIEVE OXYGENATION TO SUPPORT ORGAN FUNCTION. • RECOMMENDED TIDAL VOLUME TO BE USED IS 6-8 ML/KG OF BODY WEIGHT • FIO2 TO BE INITIALLY KEPT AT 1.0 AND THEN SUBSEQUENTLY DECREASED AS PER REQUIREMENT TO MAINTAIN PAO2 OF 60 MM HG.
MECHANICAL VENTILATORY SUPPORT • IF PAO2 CANNOT BE MAINTAINED AT 60 MM HG BY FIO2<0.6 , PEEP MAY BE ADDED.
WHAT IS PEEP? • IT IS POSITIVE END EXPIRATORY PRESSURE.
WHAT DOES IT DO? • ELEVATES MEAN ALVEOLAR PRESSURE. • PREVENTS END EXPIRATORY AIRWAY AND ALVEOLAR CLOSURE. • MAY PREVENT THE REPITITIVE AND CYCLICAL RE OPENING OF CLOSED ALVEOLI PREVENTING ALVEOLAR DAMAGE.
CAUTIONS • START FROM 5 CM H20 . • GO TO A MAXIMUM OF 20-24 CM H2O. • MAINTAIN O2 SATURATION OF >90% AND FIO2< 0.6 • MONITOR THE PULSE AND BP TO AVOID CARDIAC COMPROMISE.
OTHER MODES • INVERSE RATIO VENTILATION • PARTIAL LIQUID VENTILATION
INVERSE RATIO VENTILATION • HERE THE INSPIRATORY TIME EXCEEDS THE EXPIRATORY TIME • IT MAINTAINS A HIGHER MEAN AIRWAY PRESSURE WITH LOW PEAK AIRWAY PRESSURE COMPARED TO CONVENTIONAL VENTILATION • IT HAS THE RISK OF DYNAMIC HYPERINFLATION WITH INCREASE IN END EXPIRATORY PRESSURE.
PARTIAL LIQUID VENTILATION • HERE PERFLOUROCARBON WHICH CARRIES LARGE AMT OF O2 AND CO2 IS USED. • IT IS RADIOOPAQUE, INERT , COLOURLESS. • ITS USED IN PTS ON ROUTINE MECHANICAL VENTILATION.
MODES OF MECHANICAL VENTILATION • ASSIST CONTROL MODE VENTILATION • SIMV(SYNCHRONISED INTERMITTENT MANDATORY VENTILATION) • CPAP(CONTINOUS PSOITIVE AIRWAY PRESSURE) • PCV(PRESSURE CONTROL VENTILATION) • PRESSURE SUPPORT VENTILATION) • OPEN LUNG VENTILATION
ASSIST CONTROL MODE VENTILATION • HERE THE INSPIRATORY CYCLE IS INITIATED BY PTS INSPIRATORY EFFORT OR IF NO EFFORT IS DETECTED WITHIN A SPECIFIED TIME PERIOD THEN BY A TIMER SIGNAL WITHIN THE VENTILATOR. • EVERY BREATH DELIVERED CONSISTS OF OPERATOR SPECIFIED TIDAL VOLUME. • VENT RATE IS DETERMINED BY THE PT OR BY OPERATOR SPECIFIED BACK UP RATE. • RECOMMENDED MODE OF VENTILATION DURING INITIATION.
SYNCHRONISED INTERMITTENT MANDATORY VENTILATION • HERE PT IS ALLOWED TO BREATHE SPONTANEOUSLY IN BETWEEN VENTILATOR DELIVERED BREATHS. • MANDATORY BREATHS ARE DELIVERED IN SYCHRONY WITH THE PTS INSPIRATORY EFFORTS. • IT ALLOWS PTS WITH AN INTACT RESPIRATORY DRIVE TO EXERCISE INSPIRATORY MUSCLES BETWEEN ASSISITED BREATHS. • USEFUL MODE OF VENTILATION FOR BOTH SUPPORTING AND WEANING INTUBATED PTS.
CONTINOUS POSITIVE AIRWAY PRESSURE. • ITS NOT A TRUE SUPPORT MODE. • IN THIS ALL THE VENTILATION OCCURS THROUGH PTS SPONTANEOUS EFFORTS. • USED TO ASSESS EXTUBATION POTENTIAL IN PTS WHO HAVE BEEN EFFECTIVELY WEANED AND ARE REQUIRING LITTLE VENTILATORY SUPPORT AND IN PTS WITH AN INTACT RESPIRATORY SYSTEM FUNCTION WHO REQUIRE AN ENDOTRACHEAL TUBE FOR AIRWAY PROTECTION.
PRESSURE CONTROL VENTILATION • THIS IS TIME TRIGGERED, TIME CYCLED,PRESSURE LIMITED VENTILATION. • DURING THE INSPIRATORY PHASE, A GIVEN PRESSURE IS IMPOSED AT THE AIRWAY OPENING AND THIS PRESSURE REMAINS AT THIS SPECIFIED LEVEL THROUGHOUT INSPIRATION. • TIDAL VOLUME AND INSPIRATORY FLOW RATE ARE DEPENDENT. • RECOMMENDED MODE IN PTS WITH DOCUMENTED BAROTRAUMA , POST THORACIC SURGERY PTS.
PRESSURE SUPPORT VENTILATION. • THIS FORM IS PT TRIGGERED, FLOW CYCLED,PRESSURE LIMITED. • SPECIFICALLY DESIGNED FOR WEANING PROCESS. • INSPIRATORY PHASE IS TERMINATED WHEN INSPIRATORY AIRFLOW FALLS BELOW A CERATIN LEVEL. • PTS RECEIVE VENTILATOR ASSIST WHEN VENTILATOR DETECTS AN INSPIRATORY EFFORT.
PRONE POSITIONING DURING MECHANICAL VENTILAITON. • THIS REDUCES THE INTRAPULMONARY SHUNT THAT OCCURS AS A RESULT OF REGIONAL ATELECTASIS. • IMPROVES OXYGENATION BY CAUSING REGIONAL IMPROVEMENTS IN TRANSPULMONARY DISTENDING PRESSURES WITHOUT OVEREXPANDING ALREADY PATENT ALVEOLI.
COMPLICATIONS OF MECHANICAL VENTILATION • BAROTRAUMA • NOSOCOMIAL PNEUMONIA • OXYGEN TOIXICITY • TRACHEAL STENOSIS • PNEUMOTHORAX • HYPOTENSION,MYOCARDIAL DYSFUNCTION. • STRESS ULCERATION IN GIT • ACUTE RENAL FAILURE • CARDIAC ARRYTHIMIAS, MOYCARDIAL DYSFUNCTION.
PHARMACOLOGICAL THERAPY • USE OF GLUCOCORTICOIDS IN HIGH DOSE NOT USEFUL. • SURFACTANT THERAPY • USE OF NITRIC OXIDE.
CASE HISTORY • 25 YR OLD MALE PRESENTED WITH H/O • FEVER WITH CHILLS-3 DAYS • VOMITING- 3-4 EPISODES • IRRELEVANT TALK-1 DAY • UNCONSCIOUSNESS- 1 DAY
ON EXAMINATION • SPO2- 100% ON AIR • BP-110/70 • RR-22/MIN • PR-116/MIN • TEMP-102 F
SYST EXAMINATION • CNS- PT SEMICONSCIOUS • NECK STIFFNESS • RESPONDING INTERMITTENTLY TO DEEP STIMULI • P/A- HEPATOSPLENOMEGALY
SYST EXAMINATION • RS- AIR ENTRY EQUAL ON BOTH SIDES • NORMAL VESCICULAR BREATH SOUNDS • CUNDUCTED SOUNDS+