Download
1 / 39
551 likes | 1.27k Vues
Lecture 6 – amino acid NTs GABA Glutamate. Amino acid NTs. GABA (gamma-aminobutyric acid) – the principal inhibitory NT, found throughout the brain and spinal cord

E N D
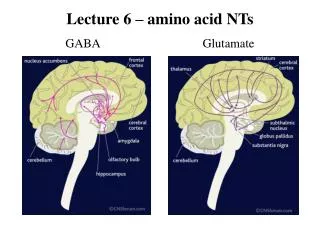
Lecture 6 – amino acid NTsGABA Glutamate
Amino acid NTs • GABA (gamma-aminobutyric acid) – the principal inhibitory NT, found throughout the brain and spinal cord • glutamate (also called glutamic acid) – the principal excitatory NT, found throughout the brain
Glutamate • the principal excitatory NT in the brain - • used in about 20% of synaptic connections between neurons • MSG = monosodium glutamate • some people experience mild neurological symptoms (dizziness, numbness) after eating food containing high levels of MSG
Glutamate • there are different sub-types of glutamate receptor, but the most studied is the NMDA (N-methyl-D-aspartate) receptor - • important role in learning & memory – responsible for initiating long-term changes in the brain associated with memory formation, • also implicated in drug addiction (especially alcoholism), • and in schizophrenia
NMDA receptor antagonists – inhibit excitatory effects of glutamate • ketamine & phencyclidine (PCP) - • have sedative & anaesthetic effects at high doses • hallucinogenic & ‘dissociative’ effects at lower doses • low dose effects replicate both ‘positive’ and ‘negative’ symptoms of schizophrenia • alcohol also acts as an NDMA antagonist
Ketamine & PCP • early studies with PCP showed it could produce an extended psychotic breakdown in some individuals, and this drug is no longer used in human research • ketamineisused in research with human subjects – although its acute effects are similar, they are less intense and have a shorter duration; adverse reactions are rare and follow-up of participants show no long-term effects (Perry et al, 2007)
Acute effects of ketamine • feeling ‘drunk’- euphoria, dizziness, nausea • disordered thought and speech • memory impairment • perceptual distortions and ‘dissociation’-objects and surroundings seem ‘unreal’ • delusional thinking - often of a paranoid nature
Instructions: Circle the number that best describes the patient’s present condition. If a specific symptom is not being assessed, circle NA. 1 = not present 2 = very mild 3 = mild 4 = moderate 5 = moderately severe 6 = severe 7 = extremely severe Brief Psychiatric Rating Scale (BPRS) 1 Somatic concern NA 1 2 3 4 5 6 7 2 Anxiety NA 1 2 3 4 5 6 7 3 Depression NA 1 2 3 4 5 6 7 4 Guilt NA 1 2 3 4 5 6 7 5 Hostility NA 1 2 3 4 5 6 7 6 Suspiciousness NA 1 2 3 4 5 6 7 7 Unusual thought content NA 1 2 3 4 5 6 7 8 Grandiosity NA 1 2 3 4 5 6 7 9 Hallucinations NA 1 2 3 4 5 6 7 10 Disorientation NA 1 2 3 4 5 6 7 11 Conceptual disorganisation NA 1 2 3 4 5 6 7 12 Excitement NA 1 2 3 4 5 6 7 13 Motor retardation NA 1 2 3 4 5 6 7 14 Blunted affect NA 1 2 3 4 5 6 7 15 Tension NA 1 2 3 4 5 6 7 16 Mannerisms and posturing NA 1 2 3 4 5 6 7 17 Uncooperativeness NA 1 2 3 4 5 6 7 18 Emotional withdrawal NA 1 2 3 4 5 6 7
BPRS scores during double-blind placebo-controlled intravenous ketamine infusion (Newcomer et al, 1999)
Ketamine & memory • studies consistently show impairment of episodic memory following sub-anaesthetic doses of ketamine, across a wide variety of tasks – • recognition memory, recall of spoken prose, recall of word lists, spatial learning, source memory tasks
GABA • the principal inhibitory NT in the brain - • used in about 40% of synaptic connections between neurons • GABA receptors are complex - • binding sites for different chemicals on the same receptor
GABA agonists • benzodiazepines, barbiturates & alcohol all enhance the inhibitory effects of GABA • these drugs all have anxiolytic, sedative & hypnotic effects • i.e. they reduce anxiety, produce physical relaxation & promote sleep
GABA antagonists • picrotoxin – a poisonous plant alkaloid with stimulant properties • flumazenil – benzodiazepine ‘antidote’ • blocks benzodiazepine site – binds but does not activate • used to treat overdose, and to reverse the sedative effects of benzodiazepines in post-operative patients
Anxiolytics • anxiolytic = drug used to reduce anxiety • barbiturates are direct GABA receptor agonists –bind to and activate GABA receptors • benzodiazepines do not directly activate GABA receptors – they enhance the effects of endogenous GABA, but GABA must also bind to receptor for drug to have effect
Barbiturates • amobarbital, pentobarbital, secobarbital, phenobarbital, etc. • first available in 1903 (Barbital) • euphoric effects of these drugs mean they have high potential for abuse, dependence & addiction • increasing dose leads to increased central nervous system depression • sedation → sleep → coma → death • pronounced respiratory depression (especially when mixed with alcohol) means high risk of fatal overdose
Benzodiazepines • first available in 1960 (Librium) • have replaced barbiturates in treatment of anxiety disorders and insomnia - • produce less respiratory depression • have pronounced sedative effect, but less euphoric • lower incidence of dependence (but may still occur in 10-30% of long-term users)
Benzodiazepines • many different benzodiazepines (BDZs) are now available - • diazepam (Valium), temazepam (Restoril), lorazepam (Ativan, Temesta), alprazolam (Xanax), midazolam (Dormicum), etc. • these differ in potency, primary effect (anxiolytic, hypnotic, muscle relaxant), time to produce effect, and duration of effect
Benzodiazepines • the most commonly prescribed psychotropic drugs in the world • estimated 20-30% of adult population are prescribed BDZ at some time • up to 5% of adult population on long-term (one year or more) prescriptions • used in treatment of anxiety disorders, insomnia, drug & alcohol withdrawal • also used as pre-anaesthetics & muscle-relaxants in surgical operations
Benzodiazepines • side-effects – • drowsiness (e.g. following day when BDZ is used for insomnia) • impaired motor co-ordination & balance • slowed reaction times • impaired vigilance task performance • impaired memory performance
Benzodiazepines & memory • effects are found mainly for long-term episodic memory – short-term memory is less affected & semantic memory is generally intact (see Curran, 1999) • studies consistently show anterograde amnesia – i.e. memory impairment for information presented after the drug has been administered • but not retrograde amnesia – i.e. no impairment for information learned before drug administration • suggests impairment of encoding processes rather than retrieval
Measuring drug effects in on-the-road driving (Verster et al 2005, Current Psychiatry Reviews 1, 215-225)
Alprazolam (‘Xanax’) & driving - Verster et al (2002) (A) Weaving (SDLP) (B) Speed variability
alcohol = any drink containing ethanol (ethyl alcohol) • produced by fermentation (conversion of sugar to alcohol by yeast) • probably the oldest recreational drug - archaeological evidence for beer & wine since about 10,000 years • acute subjective effects of alcohol are biphasic - • low doses are mildly stimulating • high doses have the opposite effect – i.e. are sedating or depressant
Biphasic effect of alcohol • BAL (U.S.) measured in grams of alcohol per 100ml of blood • BAC measured in grams per litre, or mg per 100ml (U.K.) • U.K. legal driving limit = .08g/100ml (BAL) = 0.8g/l = 80mg/100ml
Alcohol & neurotransmitters • alcohol is a pharmacologically ‘messy’ drug • acute effects on NT systems are wide-ranging and complex - • increases inhibitory NT activity (GABA) & • decreases excitatory NT activity (glutamate) • this causes knock-on effects on other NT systems throughout the entire brain
Alcohol abuse & dependence • chronic alcohol abuse leads to adaptations in physiological processes that act in opposition to drug effects in order to maintain homeostasis • sudden withdrawal of alcohol leads to rebound effects, which are opposite to the effects of drug • these are experienced as an unpleasant withdrawal syndrome,which can only be alleviated by reinstating alcohol use • so individual becomes dependent on alcohol for normal functioning
acute withdrawal effects in long-term alcoholics – • anxiety, delirium, hallucinations & potentially fatal seizures • these reflect state of excessive neural excitation • alcohol withdrawal symptoms are reduced by administering benzodiazepines (to enhance inhibitory GABA-ergic activity)
Alcohol & task performance • although acute subjective responses to alcohol are biphasic, effects on psychomotor performance appear to be linear • i.e. even low-to-moderate doses (which may be subjectively stimulating) can impair task performance • impairment in psychomotor tasks (simple & choice reaction time, vigilance) is evident before subject is ‘drunk’ and at BAC levels that are below the legal driving limit • impairment increases with increasing dose -
Effects at different blood alcohol concentrations (BAC in grams of alcohol per litre of blood)
Alcohol & task performance • performance is most affected on more complex tasks (see Kerr & Hindmarch, 1998) • so a low dose that doesn’t impair performance on simple psychomotor tasks may still have a negative effect on more complex tasks (e.g. driving) • alcohol also produces anterograde amnesia in memory tasks
Effects of 0.8g/kg alcohol on Tower of London task: ITT = log. initial thinking time, STT = log. subsequent thinking time (from Weissenborn & Duka 2003, Psychopharmacology 165, 306-312)
Alcohol & TOL task - Weissenborn & Duka (2003) • all differences are p<.05 • time to first move (ITT) is shorter in subjects given alcohol • but subsequent thinking times (STT) are longer • and fewer perfect solutions are achieved • shorter ITT may reflect increased impulsivity • mean BAC in alcohol group at time of testing was < 0.6 g/l • legal driving limit is 0.8 g/l
Glutamate & GABA - summary • glutamate - the principal excitatory NT in the brain • NMDA glutamate receptors have an important role in learning & memory, schizophrenia & addiction • ketamine – NMDA receptor antagonist that produces acute dissociation & schizophrenic-like symptoms • GABA - the principal inhibitory NT in the brain • GABA agonists (benzodiazepines, barbiturates, alcohol) have anxiolytic, sedative & hypnotic effects • benzodiazepines are the most widely prescribed psychoactive drugs in the world; used to treat anxiety & insomnia, side-effects include impaired reaction time, attention & memory • alcohol is both a GABA agonist & a glutamate antagonist • long-term alcohol abuse alters balance of inhibitory/excitatory neurotransmission, which can lead to alcohol dependence & withdrawal syndromes • acute subjective effects of alcohol are biphasic (low doses feel stimulating, high doses sedating), but even low doses can impair cognitive performance – especially on complex tasks (problem solving, driving)
Learning outcomes • Be able to describe the acute effects of ketamine intoxication, and how these are related to the ‘positive’ and ‘negative’ symptoms of schizophrenia. • Know the main conditions for which benzodiazepine drugs are prescribed, and understand the neuro-chemical basis of the therapeutic effects and side-effects of these drugs. • Understand the psychopharmacological basis for the acute effects of alcohol, and the mechanisms underlying alcohol dependence and withdrawal syndromes.
Recommended reading GLUTAMATE & KETAMINE • JW Newcomer et al (1999) Ketamine-induced NMDA receptor hypofunction as a model of memory impairment and psychosis. Neuropsychopharmacology 20, 106-118 • EB Perry et al (2007) Psychiatric safety of ketamine in psycho-pharmacology research. Psychopharmacology 192, 253-260 GABA & ANXIOLYTICS • HV Curran (1999) Effects of anxiolytics on memory. Human Psychopharmacology 14, S72-S79 • JC Verster et al (2002) Effects of alprazolam on driving ability, memory functioning and psychomotor performance. Neuropsychopharmacology 27, 260-269
ALCOHOL • JS Kerr & I Hindmarch (1998) The effects of alcohol alone or in combination with other drugs on information processing, task performance and subjective responses. Human Psychopharmacology 13, 1-9 • CF Valenzuela (1997) Alcohol and neurotransmitter interactions. Alcohol Health & Research World 21, 144-148