Download
1 / 49
611 likes | 1.55k Vues
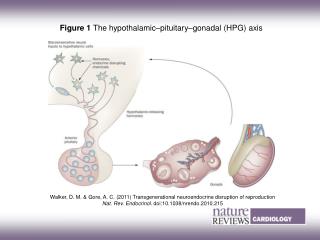
Hypothalamic & Pituitary hormones. Eric Lazartigues, Ph.D. Department of Pharmacology elazar@lsuhsc.edu (504) 568-3210. Hypothalamus-Pituitary: Anatomy. Hypothalamus: nervous tissue below thalamus Pituitary: small outgrowth of the forebrain, size of half a pea Two functional parts

E N D
Hypothalamic & Pituitary hormones Eric Lazartigues, Ph.D. Department of Pharmacology elazar@lsuhsc.edu (504) 568-3210
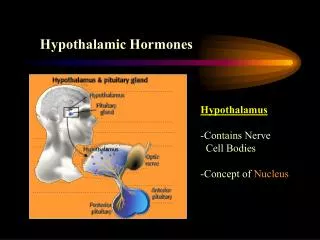
Hypothalamus-Pituitary: Anatomy • Hypothalamus: nervous tissue below thalamus • Pituitary: small outgrowth of the forebrain, size of half a pea • Two functional parts • Adenohypophysis (anterior pituitary) • Rathke’s pouch – ectoderm above mouth • Neurohypophysis (posterior pituitary) • Hypothalamus • Move together during development
Hypothalamus-Pituitary: Blood and nerve supplies • Hypothalamus • Hypothalamic neurons release hormones directly into capillary plexus • Anterior pituitary • Blood supply from median eminence of hypothalamus – portal system • Hormones from hypothalamus to pituitary • Sympathetic/parasympathetic nerves • Posterior pituitary • Supraoptic and paraventricular nuclei in hypothalamus
Serum ACTH Levels Awake Sleep Frequency 20 LH 15 amplitude mIU/ml 10 5 Ultradian 6 4 ng/ml 2 Testosterone 0 1 2 3 4 5 6 7 8 Hr • The pulsatile nature of hormone release from the hypothalamus is critical for maintained optimal responsiveness of the pituitary cells. • Pulsatile secretion decreases the extent of down-regulation of pituitary receptors. • Continuous release of hypothalamic hormones actually suppresses the secretion of pituitary hormones.
Pituitary releasing hormones • CRH: Corticotrophin releasing hormone (ACTH) • TRH: Thyrotrophin releasing hormone • GHRH: GH releasing hormone • Somatostatin: GH inhibition • GnRH: Gonadotrophin (LH, FSH) releasing hormone • Dopamine: Prolactin inhibition • Vasopressin: ACTH release
Pituitary releasing hormones • Small peptides • Active at relative high concentrations • Rapidly degraded • Low concentration in peripheral circulation • Special circulation allows high concentrations to reach targets
Feedback control Feedback STRESS, Metabolic status CNS Control Stress HYPOTHALAMUS XIH XRH Long loop Short loop (-) (+) Target Hormone (- ) T ropic Hormone T ropic Hormone PITUITARY Long loop Tropic Hormone (+ ) Target Hormone (- ) Target Gland
Thyrotrophin (TSH) • Stimulates: thyroxine synthesis thyroid growth • Regulation: • TRH: stimulates release • Inhibited by thyroid hormones (T3, T4) – feedback inhibition • Acts via cAMP
Thyroid Stimulating Hormone: TSH • Thyrotrophs: Thyroid Stimulating Hormone (TSH) • Hypothalamic Control Thyrotropin Releasing Hormone (TRH) • Target Tissue Follicular cells of the Thyroid gland • Hormone effects: controls the production of T3 and T4
Endocrine activity of the Thyroid Gland • Follicular cells: T3 and T4 • Target Tissue; Almost all body tissues • Hormone effects: Increases body metabolism Increases gluconeogenesis Increases glycolysis Increases lipolysis Increased basal metabolic rate (BMR) Increases heart rate and force of contraction
Hypothyroidism • Hypothyroidism (3% of population) endemic goiter: (due to I2 deficiency) Classification: I, II or III Treatment: Thyroxine (T4) daily (levothyroxine) or combination T3+T4 • Congenital hypothyroidism (Cretinism): 1:4000 newborns Physical and mental growth and development are greatly retarded Treatment: Thyroxine daily (levothyroxine)
Hyperthyroidism Grave’s Disease with exophthalmos • Temporary treatment: • Thyrostatics: • Methymazole: inhibit formation of T4 • Propylthiouracil: prevent conversion T4 to T3 • Beta blockers: • Metoprolol: Management of symptoms only • Permanent treatment: • Surgery: remove whole or part of thyroid • 131Iodine orally: destroy hyperactive cells Toxic multinodular goiter Toxic thyroid adenoma
Proopiomelanocortin (POMC) 1 gene, multiple hormones Oligosaccharides b -LPH ACTH biosynthetic intermediate -MSH sequences 16K Fragment ACTH b -Endorphin g -LPH Corticotrophin (ACTH) secretion
ACTH • Corticotrophs Adrenocorticotropic hormone (ACTH) • Hypothalamic Control Corticotropin releasing hormone (CRH) • Target Tissue Adrenal cortex, Zona Fasciculata • Hormone affects: control production of glucocorticoids such as cortisol
Endocrine activity of the Adrenal Cortex • Zona glomerulosa Mineralocorticoids such as Aldosterone • Hormonal control renin-angiotensin pathway permissive effect of ACTH • Target tissue: Principle cells of the DCT and collecting duct • Hormone affects: increases reabsorption of Na+ and water
Endocrine activity of the Adrenal Cortex • Hyper-secretion: Aldosteronism: Hypokalemia, increase in extracellular fluid and blood volume,and hypertension, may also have period of muscular paralysis • Hypo-secretion: Addison’s disease Mineralocorticoids deficiency, death occurs in four days to two weeks if untreated
Endocrine activity of the Adrenal Cortex • Zona Fasciculata Glucocorticoids such as cortisol and cortisone • Hormone control: ACTH • Target tissue: Liver and general body cells • Hormone affects: Stimulates gluconeogenesis by the liver Decreased glucose utilization by cells
Endocrine activity of the Adrenal Cortex • Hormone effects: Elevated blood glucose levels Reduction of protein stores in all body cells except the liver increased plasma protein levels promote lipolysis and beta oxidation of fat Helps body recover from stress Prevention of inflammation
Endocrine activity of the Adrenal Cortex • Hypo-secretion Addison’s disease - glucocorticoid deficiency person becomes highly susceptible to disease and deteriorating effects of stress ACTH stimulation test (tetracosactide) • Hyper-secretion: Cushing’s Syndrome mobilization of fat from lower body to the thoracic and upper abdominal regions giving raise to “Buffalo Torso”
Stress overcomes negative feedback regulation STRESS - Infection - Trauma - Surgery Hypoglycemia Sleep/wake - Pain, Cold CRH Cortisol HYPOTHALAMUS Short Long CRH Loop Loop ACTH Cortisol ACTH a-MSH Long Corticotroph Loop Cortisol
Anterior Pituitary Hormones: Stimulation Testing ACTH (ATHAR, COSYNTROPIN) - Not used clinically to treat adrenal insufficiency due to expense - Used for stimulation testing. ACTH (IV ACTH should result in in peak plasma levels of glucocorticoids in 3-60 min - Tx myasthenia gravis Adverse Effects (Prolonged use): Suppression of hypothalamic pituitary-adrenal axis, immunosupression, hypertension Drug Interactions: natriuretic and diuretic effects of diuretics. Use with K+- depleting diuretics can produce severe hypokalemia. Contraindications: Surgery, 1o adrenal insufficiency, heart failure TRH/TSH (Thyrotropin; recombinant human TSH (THYROGEN) Not commonly used to treat thyroid disorders but are used to distinguish between hypothalamic-pituitary-thyroid gland dysfunction.
Endocrine activity of the Adrenal Cortex • Zona reticularis Produces small amounts of androgens, mostly dehydroepiandrosterone (DHEA), DHEA may be converted into estrogens • Hormone Control: Believed to be ACTH • Target tissue: General body cells
Endocrine activity of the Adrenal Cortex • Hyper-secretion: Adrenogenital Syndrome Congenital Adrenal hyperplasia: 11b-hydroxylase deficiency (90-95%) • Salt wasting crises in infancy • virilization of female infants • Sex assignment issues and controversies
Gonadotropic hormones • GnRH:pulsatile secretion • Cyclical secretion LH, FSH • Females: ovary • LH: ovulation, corpus luteum • FSH: dvpt follicle, oestradiol and progesterone • Males: testes • LH: Leydig cells: testosterone • FSH: Sertoli cells: spermatogenesis • FSH: inhibin: negative feedback
Decapeptide half-life of 2-4 min. • Pulsatile secretion, arcuate nucleus • Continuous secretion: downregulation (clinical use) • Diagnostic use: synthetic GnRH, Gonadorelin (FACTREL) stimulation testing: pituitary can secret LH/FSH? • Therapeutic uses: • Management of infertilty: promote physiological cycle • Suppression of gonadotropin secretion: non-pulsatile • GnRH-dependent precocious puberty: before 8-9 year-old • Endometriosis, Uterine leiomyomata (fibroids) estrogen-sensitive fibrous growths • Pharmacological castration (paraphilia): triptorelin (TRELSTAR) GnRH and analogs
Side Effects (chronic non-pulsatile administration) • Females: Typical symptoms of menopause: hot flashes, sweats, headaches and bone density. Depression, libido, generalized pain, vaginal dryness, and breast atrophy may also occur. • Men: Testicular atophy, sweats, edema, gynecomastia, libido, • hematocrit, bone density, • Both: dizziness, vertigo, insomnia,, and headache • Drug-drug Interactions: • Androgen therapy: DECREASE Efficacy • Discontinue nasal decongestants • Contraindications: Pregnancy, breast-feeding, osteoporosis, undiagnosed abnormal vaginal bleeding GnRH and analogs (continued)
GnRH antagonists • Ganirelix (ANTAGON) and cetrorelix (CETROTIDE) • Mechanism of Action: Inhibit the secretion of LH>>FSH in a dose dependent manner. Administer subcutaneously • Use: Inhibit premature (LH) surges in women undergoing controlled ovarian hyperstimulation with FSH and hCG, followed by subsequent assisted insemination or reproductive technology (ART) procedures • Adverse effects: nausea and headaches. • Contraindications: primary ovarian failure, pregnancy, breast feeding • Abarelix (PLENAXIS) • Indication: Prostate cancer to prevent adverse consequences of tumor growth. Distribution limited (hypersensitivity reactions).
Clinical use of FSH/LH • Diagnostic uses: • a. Pregnancy:hCG detection in urine or plasma • b. Timing of ovulation: occurs 36 hours after the onset of LH surge • c. Diseases of Male and Female Reproductive Systems • Low LH and FSH: hypogonadotrpoichypogonadism : hypothalamic or pituitary disease • High LH and FSH: primary gonadaldiseases • Therapeutic Uses of Gonadotropins: • Purified from the urine of pregnant women or postmenopausal women • hCG (PREGNYL, NOVAREL, PROFASI…) mimics action of LH • Menotropins (PERGONAL, REPRONEX): equal amount LH and FSH • Recombinant FSH: rFSH: follitropina (GONAL-F) and follitropinb (PUREGON, FOLLISTIM) • Female infertility in combo with ART: Anovulation, Polycystic Ovary disease • Adverse effects: multiple pregnancies and ovarian hyperstimulation syndrome (OSS) • Male Infertility Secondary to gonadotropindeficiency, cryptorchidism • Most common side effect is gynecomastia
Prolactin • Secreted by lactotrophs • Lactation • Inhibits reproductive hormone secretion • Release inhibited by dopamine • Animals: osmoregulation, growth • Stalk transection prolactin • No therapeutic use • Hyperprolactinemia: • Women: galactorrhea, amenorrhea, infertility • Men: loss of libido, impotence, infertility • Rx: surgery, radiation, D2 agonists
Pharmacological Treatment of Prolactin excess: DA agonists Bromocriptine interacts with D2R on lactotrophs - Note only 7% reaches circulation do first-pass metabolism by the liver. Longer acting version (PARLODEL-LAR) – Pergolide(PERMAX) off label treatment Cabergoline (DOSTINEX) ergoline-derived dopamine agonist .More potent and longest half-life Mechansism of Action: Shrink pituitary PRL-secreting tumors, lower circulating PRL levels, and restore ovulation in approximately 70% of women with microadenomas and 30% of women with macroadenoma Side Effects: Nausea, headaches, orthostatic hypotension Drug-drug Interactions: May effects of anti-hypertensives, and effectiveness of dopamine antagonists such as the antipsychotics and the phenothiazine-type antiemetics
Growth hormone • Promotes growth: skeleton, muscles, viscera • Effects mediated by somatomedins (e.g. IGF1, 2...) • Released at night during growth • Variety of metabolic effects • Anabolic, positive nitrogen balance • Anti-insulin • Stimulated by GHRH, stress, exercise • Inhibited by somatostatin
Physiological Effects of GH Increased Organ and Tissue growth Protein Synthesis Gluconeogenesis Increased Glucose Uptake Glucose Uptake Fat deposition Protein Synthesis
Growth Hormone Deficiency Children: Dwarfism. Most common is isolated idiopathic • Insulin-stimulated hypoglycemia induced GH < 10 µg/L • Exclude nutritional deficiencies • Height ≥ 2–2.5 SD below normal, delayed bone age. Adults > 90% have overt pituitary hypofunction due to disease, pituitary adenoma or iatrogenic • Insulin-stimulated hypoglycemia induced GH < 3 µg/L 9 year old Peruvian girl (80 cm) with GH receptor defect
Clinical Uses of Recombinant Human Growth Hormone Primary Therapeutic Objective Clinical Condition Growth Growth failure in pediatric patients : Growth hormone deficiency Prader-Willi syndrome Turner syndrome Small for age with failure to catch up by age 2 Idiopathic short stature in pediatric patients Improved metabolic state, Growth hormone deficiency in adults lean body mass, sense of well-being lean body mass, weight, AIDS-related muscle wasting and physical endurance Improved GI function Short bowel syndrome in patients receiving specialized nutritional support
Treatment of GH insufficiency (all SC or IM) : • GH SUPPLEMENTATION • Somatropins GH preparations whose sequence matches native hGH. • Somatrem: GH derivative with an additional methionine at the amino terminus. • Side effects: hyperglycemia (may be contraindicated in diabetes) and increased intracranial pressure. • Additional approved uses of GH therapy: “Social use” short stature within “normal” ranges, bodybuilding, athletes, ageing. • GHRH LIKE ACTIONS • sermorelin peptide that corresponds to the first 29 amino acids of GHRH. • - Used diagnostically to Decrease serum GH levels • - Tx Children with 3o (hypothalamic deficiency) • Side effect: angina, flushing • IGF-1 THERAPYFor Pts with GH Receptor mutation • Mecasermin: complex of recombinant human IGF-1 (rhIGF-1) and recombinant human insulin-like growth factor-binding protein-3 (rhIGFBP-3). • Clinical response is monitored Serum IGF-1 levels.
Growth hormone release Acromegaly Normal 06:00 12:00 18:00 24:00 06:00
Growth Hormone Excess • Hyper-secretion: • During childhood causes • Gigantism (up to 8 – 9 ft.) • During Adulthood causes • Acromegaly: • Enlargement of the small bones of the hand and feet • Enlargement of the cranium, nose, and lower jaw • Tongue, liver, and kidneys become enlarged • Periosteal Bone growth • Excess soft tissue • Enlarged organs. • Cardiomyopathy • Often diabetic • Infertile? GH ~ PRL Don Fermin y Urieta (1870-1913) “The Giant of Aragon” 229 cm tall
SOMATOSTATIN (SS) ANALOGS Drug Type Dosing OctreotideShort-acting Subcutaneous 3 times/day; dose range of 50-500 mg Octreotide LAR Long-acting Intramuscular every 28 days; dose range of 10-40 mg Lanreotide depot Long-acting Intramuscular every 7-14 days Lanreotideautogel Long-acting Deep subcutaneous every 28 days Octreotide(SANDOSTATIN) 8 amino acid derivative of somatostatin that preferentially binds to SS receptors on GH-secreting tumors. Lanreotide (SOMATULINE-LA) slow release, long-acting octapeptide causes prolonged GH suppression. Most effective for patients with non-pituitary tumours Side effects: Inhibits gastrointestinal and pancreatic function Long-term use causes digestive problems such as loose stools, nausea, and gas ~ 25% of patients develop gallstones Arrhythmias, sinus bradycardia, and conduction disturbances Drug Interactions: Cyclosporine bioavailability
DOPAMINE-RECEPTOR AGONISTS(see Prolactine section) • - Bromocriptine (Parlodel) • Cabergoline. (DOSTINEX) Long-acting oral agonist • Paradoxically reduce GH secretion from pituitary tumors • Side effects: nausea and hypotension • Contraindications: Patients with hypertensive • disorders of pregnancy (preeclampsia, eclampsia) GROWTH HORMONE ANTAGONISTS: Pegvisomant (SOMAVERT) GH analog binds receptor but does not induce receptor dimerization or Jak/Stat signaling. Adverse Effects: No negative feedback at the pituitary or hypothalamus: May endogenous GH levels. May also see excessive tumor growth. Contraindications: IV therapy, breast feeding
Posterior pituitary hormones (1) • Vasopressin/Antidiuretic hormone (ADH) • Produced by SON and PVN magnocellular neurons • Conserves water - concentrates urine • Water reabsorption by collecting tubule • Deficiency: diabetes insipidus • Extreme thirst and polyuria • plasma sodium and osmolality • Excess: inappropriate ADH “water intoxication” (SIADH)
Diseases Affecting the Vasopressin System • AVP hyposecretion: • Diabetes insipidus: large volume of diluted urine • Central DI: insufficient secretion (trauma HP axis, idiopathic) • Rx: Desmopressin: increase urine osmolality (test vs. NDI) • Chlorpropamide (oral sulfonylurea): potentiates low AVP • Carbamazepine and clofibrate (rarely): reduce polyuria • Nephrogenic DI: insufficient response (congenital or acquired) • Many forms are drud-related: lithium • X-linked NDI: mutation V2 receptor gene • Autosomal recessive and dominant NDI: mutation aquaporin 2 • Rx: Amiloride: blocks uptake of Lithium • Thiazide: non-lithium related DI: reduce polyuria • Indomethacin: (?) decrease PG and enhance AVP effects
Diseases Affecting the Vasopressin System • AVP hypersecretion: • SIADH: impaired H2O excretion, hyponatremia, hypo-osmolality • Causes: malignancies, lung/CNS diseases • Psychotropic , sulfonylureas, vinca alkaloids: Drug-induced SIADH • Rx: water restriction, hypertonic saline, loop diuretics • Demeclocycline: inhibit AVP action in collecting ducts • Lithium: mild efficacy, irreversible damages (chronic), low TI • Other water retaining states: • Congestive HF, cirrhosis, nephrotic syndrome: hypovolemia • hypovolemia→AVPrelease→hyponatremia • Need for orally active V2 receptor antagonists
Posterior pituitary hormones (2) • Oxytocin • In the periphery: • Milk let-down • Uterine contraction • Sexual intercourse (orgasm ?) • In the brain: • Sexual arousal • Bonding • various behaviors, including social recognition, bonding, anxiety, trust, and maternal behaviors.
Oxytocin Uterus Contractions Breast: milk ejection Clinical Use of OXYTOCIN Induction of labor –oxytocin (PITOCIN,) is treatment of choice to induce labor. Due to short half-life it is given as IV drip -(start at 2-10 mU/min then increase up to 2 mIU/min at 20-min intervals. If doses of 40 mIU/min fail, higher rates of infusion are unlikely to be successful. Continuous monitoring of fetal and maternal HR, BP and strength of uterine contraction is required. Due to structural similarity to AVP, high doses may have pressor and anti-diuretic activity c. 3rd stage labor and Puerperium: Oxytocin is given following delivery of fetus to help maintain uterine contractions- this greatly reduces the incidence and extent of hemorrhage. -positive feedback - participates in parturition but not required Stretch
Oxytocin (PITOCIN) Mechanism of Action : Acts on G-protein coupled receptors in the myometrium Increase intracellular Ca2+ Increase prostaglandins Increase gap junctions Net effect: Increased rate and force of myometrial smooth muscle contraction Side Effects: Hypersensitive uterine reaction: Increased, hypertonic uterine contractions, resulting in cervical laceration, postpartum hemorrhage, pelvic hematoma, and uterine rupture Drug Interactions: Cannot be used with vasopressors Effectiveness is general anesthetics Contraindications: Immature fetal lungs, Evidence of fetal stress (oxytocin challenge test), abnormal fetal position. Use of oxytocin during pregnancy can precipitate uterine contractions and abortion
Suppression of Preterm Labor Preterm (premature) labor begins before the 37th week of pregnancy. Tocolysis: The delaying or inhibition of labor during the birth process. -adrenergic agonists Ritodrine L-type Ca2+ channel blockers; Nifedipine Oxytocin-Receptor Antagonists (atosiban) Peptide analogs that competitively inhibit the oxytocin receptor. Decreases frequency of uterine contractions and increased the number of women who remained undelivered, Comparable efficacy to adrenergic agonists but with a lower incidence of side effects.