Download
1 / 22
220 likes | 429 Vues
Lyme Borreliosis Helen Winslow Helen Winslow is a registrar in infectious diseases and tropical medicine at Royal Liverpool and Broadgreen University Hospitals NHS Trust. She has a particular interest in the health of returning travellers. Lyme Borreliosis Learning Objectives Introduction

E N D
Lyme Borreliosis Helen Winslow Helen Winslow is a registrar in infectious diseases and tropical medicine at Royal Liverpool and Broadgreen University Hospitals NHS Trust. She has a particular interest in the health of returning travellers. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment This module provides a summary of the presentations of early and late Lyme disease, its treatment, the approach to determining the risk of Lyme disease and the concerns regarding Post-Lyme syndromes.
Learning Objectives • By the end of this session you will be able to: • Outline how a history of tick bite or potential exposure in different geographic areas forms part of the picture informing clinicians of the likelihood of Lyme as clinical possibility. • Illustrate the differing presentations of early and late Lyme disease. • Define key diagnostic methods and when they are indicated. • List the evidence for treatment at each stage including the approach to 'Post-Lyme syndromes’. • Explain prevention strategies and the indications for prophylactic antibiotic treatment. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Introduction Lyme borreliosis is a multisystem disease caused by the spirochete BorreliaBurgdorferi which is transmitted to humans through Ixode tick bites. Found across Europe, Northern America and temperate Asia, it is most commonly seen in people who work or spend leisure time in rural areas. This session starts by looking at the probability of Lyme disease in patients depending on geographic location, activity and season. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment It examines the common presenting features of early localised and disseminated borreliosis before going on to cover the features of late infection as well as considering the gaps in evidence explaining the 'Post-Lyme Syndrome' that some patients report. The session will review the diagnostic methods and evidence based treatment strategies before concluding with ways to reduce the chance of contracting Lyme infection and indications for prophylaxis.
Transmission of Lyme Disease In the Northern hemisphere Lyme Borreliosis is the most common disease carried by ticks. It is estimated that there are between 20 and 100 cases per 100,000 people in the US and 100 to 130 cases per 100,000 in Europe. Numbers are increasing each year. Knowledge about the transmission of Lyme disease, activities that place people at risk and geographic variation in the carriage of BorreilaBurgdoferiare important to clinicians in order to determine the possibility of Lyme disease as a cause of symptoms which may appear weeks or months after a tick bite. Lyme illness has become a cause of great anxiety to some patients because of the links that have been made between chronic fatigue syndrome and • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment previous or presumed Lyme infection (by some physicians and patient groups). In previously untreated patients, the risk of Lyme exposure should be explored to allow appropriate investigation if present. Ruling out exposure risk can be important in order to pursue other diagnostic/treatment avenues for disabling symptoms.
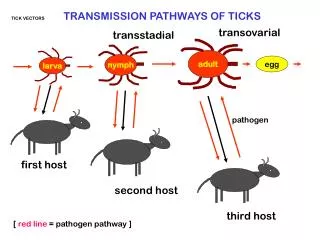
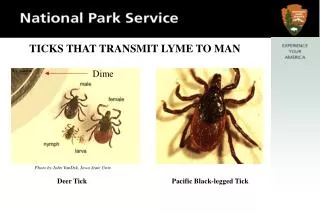
Ticks I • Ixode ticks, of which 5 types have been shown transmit BorreilaBurgdoferi globally, are carried mainly on deer and sheep. However, they also feed on small mammals and birds which form a natural resevoir for Borrelia species. The spirochetes are harboured in the stomachs of infected ticks and are transmitted onward, not on attachment but when the tick begins to feed between 24 and 72 hours later. Ticks develop through: • Larval stages (uninfected) • Nymph stages (low rates of infection) • Adult (highest rates of infection) • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment Life cycle of an Ixode tick
Ticks II • Ixode ticks reproduce mainly between May and September (in the northern hemisphere). As a result, risk of Lyme transmission is highest: • After activities in tick infested areas. This particularly includes wood and • moorland but also potentially any habitat in which there are deer and sheep. • In summer, when most acute cases are seen. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Factors • The risk from a recognised bite is dependent on a series of factors including: • Tick species • Stage in lifecycle • Time duration of attachment • Geographic location • There is huge variation in the the prevalence of Borrelia carriage in Ixode tick populations around the world. In some areas of New England this can be as high as 50% in adult ticks - meaning each bite poses a serious risk of Lyme. Carriage rates above 20% are seen in significant areas of the eastern US and pockets of continental Europe. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment • Manifestations of Lyme disease vary geographically depending which of the four pathogenic subtypes of BorreliaBurgdorferi is responsible: • Afezelii • Garinii • SensuStrictu (US) • Spielmanii RIGHT: US map shown areas of known Lyme transmission
Presentation • Recognising varying presentations is important because three distinct groups of symptoms exist. Correct identification prompting appropriate treatment results in complete resolution of symptoms in 90-95% of patients: • Early localised disease: The erythemamigrans rash and viral type illness. • Early disseminated disease: Most commonly affecting the nervous system. • Late disease: This can involve the central and peripheral nerves, arthritis • and a cognitive component. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Rash • An ErythemaMigrans rash is the most common early sign of BorreliaBurgdorferi infection occurring in 60-80% of cases. • Usually, but not always, around the site of the inoculating tick bite, this is a round red lesion often with central clearing and should be over 5 cm in diametre with a supporting history in order to be pathognomonic. Points to remember: • Typically appears 1-2 weeks after removal of the tick, although this can • range between 3 and 30 days. • It doesn't itch or hurt. • Lesions usually start small and expand over a few days before fading over a • period of about one month. • Solitary lesions are most common but these can be multiple • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment Bull eye type rashes in joint folds or beneath underwear that would be unusual for cellulitis should always prompt a thorough history to elicit risk of contact with ticks.
Disseminated Early Infection • Neuroborreliosis is seen in 10-15% of cases that have not previously received treatment courses of antibiotics. • There is significant variation in the likelihood of specific neurological features depending on the BorreilaBurgdoferi subtype. • Most common presentations include: • Meningitis- which maybe insidious or subacute • Radiculopathy (Bannworth's syndrome) • Cranial nerve palsies, most commonly being a 7th cranial nerve palsy which may be bilateral. These often are associated with a lymphocytic CSF with or without symptoms or meningism. • Meningioencephalitis, ocular signs including episcleritis and conjunctivitis and peripheral neuropathies may also occur in early infection but more rarely. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Lyme Carditis Lyme carditis can take the form of either atrioventricular block or pericarditis. Patients with any evidence of heart block thought to be due to early Lyme infection should be admitted and monitored in hospital as this may worsen rapidly and necessitate cardiac pacing. Patients with symptomatic myo or pericarditis should be cared for similarly. These also present within a few weeks to several months of infection. Borreliallymphocytoma is another rarer sign of early manifestation which may develop at the site of antecedent tick bite particularly if this happened to occur on an ear or the scrotum. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment RIGHT: ECG showing different types of heart block as can occur with Lyme carditis.
Late Neuroborreliosis If left untreated, symptoms of chronic Lyme disease may develop. Late neuroborreliosis usually presents as an encephalomyelitis and can resemble multiple sclerosis. Patients typically present with mild positive and negative sensory symptoms, mild paraesthesias, sensory loss, gait instability but minimal weakness. It is important to remember that all early and late symptoms are caused by active infection. As a result, resolution of symptoms or significant improvement is expected in response to antibiotic treatment. Underlying tissue damage may be residual but the development of new or further symptoms after an adequate treatment course is not expected. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Diagnostic Techniques I Whilst many early presentations of Lyme can be diagnosed clinically, the symptoms common in later stages are not exclusive to Borreliosis. Accurate and validated diagnostic testing is therefore important. BorreliaBurgdorferi antibody develops within a 4 to 8 week period after initial infection and often remains positive for years. Antibody testing in early disease therefore has low positive rates but this increases to over 99% in late cases. Negative results from accredited laboratories are therefore very useful and should prompt pursuit of other diagnostic possibilities unless pretest clinical suspicion is very high. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Diagnostic Techniques II It is generally agreed that neurological presentations of suspected Lyme should undergo investigation including CSF analysis. 90% of early neuroborreliosis cases have detectable intrathecal antibody. PCR of body fluids for detection of Borrelial DNA can be a useful diagnostic • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment tool especially in Lyme arthritis. Yields are highest in synovial fluid and reduce in CSF (in both early and late neurological presentations). They are reduced further with skin biopsy in acrodermatitis and migrans rash and are lowest in blood, in which PCR rarely produces useful results. Borrelial culture is possible but rarely done in non-research settings.
Management options I • There is good evidence to support the use of doxycycline, amoxicillin and third generation cephalosporins for the treatment and cure of Lyme disease. • Antibiotic choice and duration are dependent on stage of: • Infection • Location of infection • Allergy and patient type • Early localised disease usually presenting with migrans rash but without neurological features or those of carditis, can be effectively treated with a two week course of oral antibiotics: • Doxycycline 100mg twice/day • Amoxicillin 500mg three times/day • Cefuroximeaxetil 500mg twice/day • Whilst IV cephalosporin can be used the two regimes above are highly effective with less risk of adverse side effects. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment Doxycycline is contraindicated in pregnancy, breastfeeding and children under 12.
Management options II • EARLY LYME • It is generally agreed that intravenous neuro-penetrative, effective antibiotics are required to treat all stages of neuroborreliosis. Length of treatment varies between studies resulting in a range of suggested durations. • Good trial evidence exists for: • 2g Ceftriaxine IV for 14 days (10-28 days) • The same should be used in Lyme carditis • There is emerging evidence that oral doxycycline is equally effective • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment • LATE LYME NEUROBORELLIOSIS • 2g IV Ceftriaxone 2-4 week duration. • Be aware that the response may be slow or incomplete. • LYME ARTHRITIS • Oral antibiotics as for local disease (doxycycline 200mg for a total of four weeks is first choice).
Post-Lyme Syndromes • There is significant debate regarding the nature of symptoms that some patients with treated Lyme disease seem to experience. A small minority patients in this group report high rates of: • Fatigue • Arthritis • Muscle pain • Memory and cognitive problems • There is a movement of patients and physicians who attribute these subjective symptoms to 'Chronic Lyme Disease'. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment • Chronic Lyme Disease: • So far no evidence of on going Borrelia infection has been identified in this cohort using validated testing methods. • After initial treatment, there is no evidence that prolonged courses of antibiotics result in any benefit compared to placebo. • Whilst there is, as yet, no universally accepted definition of Post-Lyme syndrome, it is accepted that this group of patients have a distressing and disabling set of symptoms. Advances in this area will be welcomed.
Prevention • Prevention is invariably better than cure. The most effective approach to prevent Lyme is the avoidance of tick bites using protective clothing and tick repellants. • ADVICE • Advice to those spending time in at risk areas is to check themselves and clothes, carefully and promptly, to minimise the likelihood of unnoticed ticks remaining attached. • Removing ticks in the first 24 hours before they begin to feed reduces transmission in both European and American settings. • EDUCATION • Education of the general population as well as medical staff aims to prompt early presentation and the correct treatment in order to minimisesequelae more common after advanced disease. • Clinicians also need to remember the possibility of co-transmission of other tick borne infections as dual pathology may result in an atypical clinical presentation and alter treatment options. Consider: • Anaplasmosis • Babesiosis • Q fever • Tick-borne encephalitis • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Prophylaxis and Vaccines There is limited evidence in this area but meta-analysis of a small number of studies suggests that prophylactic antibiotics given within 72 hours of a bite, reduce the incidence of subsequent Lyme from 2% to 0.2% NNTI 50 (these were done in the US where ticks analysed show a carriage rate of BorreliaBurgdorferiof >20%). This can be achieved with a single dose of doxycycline 200mg or 10 days of amoxicillin if the former contraindicated. A vaccine preventing the development of Lyme has been withdrawn due to unfounded public fears of autoimmune side effects. The development of alternatives is underway and would provide useful protection for people most at risk of bites from carrier ticks. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Key Points • The degree of clinical suspicion of Lyme disease is dependent on exposure history of a patient which clinicians should elicit. • Common early presentations include a chronicummigrans rash with or without viral type illness. Presence following a bite warrants treatment without serological evidence. • Neurological manifestations are seen in a significant proportion of early disseminated disease. Lyme must be considered as a cause for unexplained peripheral neuropathies, cranial nerve palsies, meningitis and encephalitis. • Treatment with appropriate antibiotics has excellent rates of cure even in late disease. • Post-Lyme syndromes have not been well explained and there is currently no good evidence suggesting that prolonged antibiotics improve symptoms. • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Summary • Having completed this session you will now be able to: • Outline how a history of tick bite or potential exposure in different geographic areas forms part of the picture informing clinicians of the likelihood of Lyme as clinical possibility. • Illustrate the differing presentations of early and late Lyme disease. • Define key diagnostic methods and when they are indicated. • List the evidence for treatment at each stage including the approach to • 'Post-Lyme syndromes’. • Explain prevention strategies and the indications for prophylactic antibiotic • treatment • Further Reading and References • P Hildenbrand et al, Lyme neuroborreliosis – Manifestations of a rapidly emerging zoonosis. American Journal of Neuroradiology, 2009;30:1079-1087. • Both perspectives regarding the existence of 'Post Treatment Chronic Lyme Disease' are explored in Clinical Infectious diseases, 2007:Jul 15;45 (2). • The Infectious Diseases Society of America has a useful evidence based set of guidelines outlining the treatment of Lyme Disease. • Information about distribution of new cases and geographical risk: • Health Protection Agency in the UK • European Centre of Disease Prevention and Control • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment
Question 1 • Lyme Borreliosis • Learning Objectives • Introduction • Transmission • Ticks • Factors • Presentation • Rash • Early Neuroborreliosis • Lyme Carditis • Late Neuroborreliosis • Diagnosis • Management • Post-lyme syndromes • Prevention • Prophylaxis • Key points • Summary • Self assessment Select the single best answer from the options given. Click on the answer to see if it is correct and read an explanation. Which of the following is not a presenting feature of Lyme disease? Presentation with tick in situ Collapse Bullseye type rash Chest Pain Ophthalmoplegia due to 6th cranial nerve palsy