Download
1 / 53
570 likes | 777 Vues
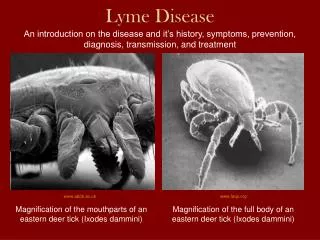
Lyme disease Lyme borreliosis. is caused by the tick-borne spirochete Borrelia burgdorferi. Lyme disease. B. burgdorferi is transmitted by ticks of the Ixodes ricinus complex including: Ixodes scapularis in north-east and north-central USA, Ixodes pacificus on the west coast of the USA,

E N D
Lyme disease Lyme borreliosis • is caused by the tick-borne spirochete Borrelia burgdorferi
Lyme disease • B. burgdorferi is transmitted by ticks of the Ixodes ricinus complex including: • Ixodes scapularis in north-east and north-central USA, • Ixodes pacificus on the west coast of the USA, • Ixodes ricinus in Europe, • Ixodes persulcatus in Asia
Lyme disease • Although cases have occurred at all ages, individuals who are active outdoors in spring and summer months are at greatest risk
Lyme disease-DEFINITION • A systemic, tick-borne disease with manifestations: dermatologic, rheumatologic, neurologic, cardiac abnormalities.
Lyme disease • The initial skin lesion, erythema migrans, is the best clinical marker (occurs in 60–80% of patients)
Lyme disease • The illness usually begins in summer with a characteristic expanding skin lesion, called erythema migrans (EM), that occurs at the site of the tick bite. • Within several days to weeks the spirochete may spread to many other sites, particularly to other skin sites, the nervous system, the heart, or the joints.
EM • The interval between tick bite and appearance of EM varies from a few days to a month (median 7 days). • The lesion begins as an erythematous papule and expands over several days to achieve a median diameter of 15cm; favored sites are the groin, buttock, popliteal fossa and axilla • A solitary lesion must measure at least 5cm;
EM • The lesions of EM are generally annular with a sharply demarcated outer border and an erythematous or bluish hue
Erythema migrans (EM) • Skin lesion typically begining as a red macute/papule and expanding over days or weeks to form a large round lesion, often with partial central clearing • The expanding EM lesion is accompanied by other acute symptoms, particularly fatigue, fever, headache, mildly stiff neck, arthralgias and myalgias.
Lyme disease- definition • 1. Erythema migrans present or • 2. At least one late manifestation and laboratory confirmation of infection
Laboratory confirmation • Isolation of the spirochete from tissue or body fluid • Detection of diagnostic levels of IgM or IgG antibodies to the spirochete in the serum or the CSF
Lyme disease • The antibody response to B. burgdorferi develops slowly. • The specific IgM response peaks between the third and the sixth week of infection. Generally IgM antibody falls to the normal range by 6 months, but occasionally it may remain elevated for much longer • The specific IgG response develops gradually over months.
Early disseminated disease • Within several days of the appearance of EM, many patients develop evidence of dissemination of their infection by the appearance of prominent systemic symptoms, the occurrence of multiple secondary skin lesions, or both. • Malaise, fatigue, lethargy, headache, fever and chills, arthralgia and myalgia are particularly common, each occurring in one-half or more of patients.
Early disseminated disease • Secondary skin lesions may occur anywhere on the body and resemble primary lesions but are usually smaller, show less expansion with time and lack indurated centers
Disseminated disease • After resolution of the signs and symptoms of early disease, some patients (20% in one series) experience a long-lasting spontaneous remission. • Most, however, subsequently develop other disease manifestations, with predominant involvement of the heart, nervous system and joints.
Early Disseminated diseaseNeurologic manifestations • cranial neuropathy (particularly Bell's palsy), • meningitis, • radiculoneuropathy, • myelopathy • encephalopathy Neurologic symptoms generally began a few weeks after EM (median 4 weeks), although some patients presented with neurologic manifestations alone. • .
Early manifestations Cardiovascular system • high-grade (2nd or 3rd degree) antrioventricular conduction or bundle-branch block defects generally resolves spontaneously in a few weeks or sooner, even in untreated patients. • myocarditis
Early Disseminated diseaseArthritis • Most people who have untreated Lyme disease develop arthritis. • Arthritis occurs in 60% of patients in the USA, at a median of 6 months after EM as disseminated disease.
Early Disseminated disease-Arthritis monoarticular or oligoarticular inflammatory arthritis involving large joints, particularly the knee
Late Lyme disease • Late Lyme disease reserved for those patients who have symptoms that persist for longer than 1 year, generally involves persistent inflammation in the CNS, joints or skin (ACA).
Late (persistent) diseaseLate neurologic syndromes • lymphocytic meningitis, • peripheral neuropathy • cranial neuritis, known as Garin-Bujadoux-Bannwarth (MPN-GBB) or Bannwarth's syndrome
Late (persistent) diseaseChronic arthritis • Arthritis becomes chronic in 20% of patients who have untreated Lyme disease, resulting in a syndrome that is clinically indistinguishable from other forms of monoarticular or oligoarticular inflammatory arthritis. • The knee is by far the most commonly affected joint.
Late (persistent) diseaseChronic arthritis • Even chronic Lyme arthritis may eventually remit spontaneously. Only a minority of patients develop radiographic evidence of erosions of cartilage or bone.
Late (persistent) diseaseChronic skin involvement • Chronic skin involvement (acrodermatitis chronica atrophicans) as a late manifestation of Lyme disease occurs primarily in Europe. • It usually occurs on the acral portion of an extremity and is characterized by violaceous discoloration and swelling of involved skin, often at a site where EM occurred years earlier.
Late (persistent) diseaseChronic skin involvement • Other clinical manifestations include: fibrotic nodules, ulnar bands, sensory disturbances, muscular weakness, myalgias, arthalgias . lichen sclerosis and atrophicus or morphea-like lesions
Late manifestations Nervous system • Lymphocytic meningitis, • Cranial neuritis, particularly facial palsy (may be bilateral), • Radiculoneuropathy • Encephalomyelitis (must be confirmed by evidence of antibody production against Borrelia burgdorferi in CSF, shown by a higher titer of antibody in the CSF than in serum)
Late disseminated disease-Carditis • - congestive heart failure • - dilated cardiomyopathy
Diagnosis Detection of a specific immune response to B. burgdorferi remains the best means of confirming the diagnosis of Lyme disease.
Diagnosis • Both immunofluorescence (IFA) and ELISA have been used to detect this antibody response • Serology results may be falsely positive or negative for various reasons, so the diagnosis of Lyme disease cannot be made by serologic test results alone. Immunofluorescence and ELISA may yield false-positive results because of epitopes in the test antigen preparations that cross-react with other bacteria.
Diagnosis • Specificity is increased by a two-step approach in which all positive ELISA results are confirmed by Western immunoblotting-to detect specific proteins in samples.
WESTERN BLOT CRITERIA • An IgM blot is considered positive if two of the following three bands are present: 24kDa (OspC), 39kDa (BmpA) and 41kDa (Fla) • An IgG blot is considered positive if five of the following 10 bands are present: 18, 21 (OspC), 28, 30, 39 (BmpA), 41 (Fla), 45, 58, 66 and 93kDa
WESTERN BLOT CRITERIA • When Western immunoblot is used in the first 4 weeks of illness, both IgM and IgG procedures should be performed. • After the first 4 weeks of illness, IgG alone should be performed.
WESTERN BLOT CRITERIA • Measurement of immunoreactivity in CSF is a useful adjunct in the diagnosis of CNS Lyme disease.To have diagnostic value, a CSF index should be calculated comparing the ratios of specific antibody to total immunoglobulin in CSF and serum
Early disseminated disease treatment • If antibiotic therapy is initiated early in the course of Lyme disease, EM typically resolves promptly and later stage disease is prevented
Early disseminated disease treatment • Early localized limited to a single skin lesion and early disseminated disease infection with mild or no systemic symptoms: -amoxicillin (500mg q8h), -doxycycline (100mg q12h) - cefuroxime axetil (500mg q12h) for 2–3 weeks.
Early disseminated disease treatment • Doxycycline, 100mg po, q12h for 21 days, or • Amoxicillin (with or without probenecid) 500mg, q8h for 21 days, or • Erythromycin, 250–500mg po, q6h for 21 days, or • Azithromycin 500mg daily for 7 days, or • Cefuroxime axetil, 500mg po, q12h for 21 days Erythromycin and azithromycin are less effective than other choices
Lyme arthritistratment • Initial treatment: • Doxycyline, 100mg po, q12h for 30 days, or • Amoxicillin and probenecid, 500mg each po, q6h for 30 days • If initial treatment fails: • Penicillin G, 20 × 106 IU iv, daily in divided doses for 14 days, or • Ceftriaxone sodium, 2g iv, daily for 14 days
Neurologic manifestationstreatment • For facial nerve paralysis alone: • Doxycycline, 100mg po, q12h for 21–30 days, or • Amoxicillin, 500mg po, q8h for 21–30 days
Lyme encephalimeningitis, radiculopathy-treatment • • Ceftriaxone, 2g iv, daily for 30 days, or • • Penicillin G, 20 × 106 IU iv, daily in divided doses for 30 days Possible alternatives: • • Cefotaxime sodium, 2g iv, q8h for 30 days, or • • Doxycycline, 100mg po, q12h for 14–30 days, or • • Chloramphenicol, 1g iv, q6h for 14–30 days
Lyme carditistreatment • • Ceftriaxone, 2g iv, daily for 14 days, or • • Penicillin G, 20 × 106 iv, daily in divided doses for 14 days Possible alternatives: • • Doxycycline, 100mg po, q12h for 21 days, or • • Amoxicillin, 500mg po, q8h for 21 days
Pregnancy • Case reports have provided convincing evidence that B. burgdorferi can cross the placenta. • Stillbirth and neonatal death have been attributed to B. burgdorferi transmitted from mother to fetus in utero, but the evidence to support this conclusion is still incomplete.
During pregnancy • Localized, early disease: • Amoxicillin, 500mg po, q8h for 21 days • Other manifestations: • Penicillin G, 20 × 106 IU iv, daily in divided doses for 14–30 days, or • Ceftriaxone, 2g, daily for 14–30 days
PREVENTION Single dose of oral doxycycline (200mg) within 72 hours after removal significantly reduces the incidence of Lyme disease in the endemic regions if the risk of transmission following tick bites is greater than 0.01.
Tick-born encephalitis (TBE) • It is transimitted by the bite of several species of infected ticks, including Ixodes scapularis, Ixodes ricinus and Ixodes persulcatus or (rarely) non-pasteurized milk of infected cows.
TBE • TBE is caused by tick-borne encephalitis virus, a member of the genus Flavivirus in the Family Flaviviridae. • Three virus sub-types are described: -European TBE orWestern TBE -Siberian TBE -Far-Eastern TBE (Russian SpringSummer encehalitis virus).
TBE • TBE manifests as: • -meningitis • -encephalitis • -meningiencephalitis.
TBE • The inculation period is between 7 and 14 days and is asymptomatic. • Shorten incubation times have been reported after milk-borne exposure.
TBE • TBE cases occur during the highest period of tick activity (between April and November).