Download
1 / 29
290 likes | 1.75k Vues
Clostridium Introduction. Clostridia are obligately anaerobic endospore-forming Gram positive rods

E N D
1. Obligately anaerobic Gram positive endospore-forming rods Clostridium
Refer to �Introduction to anaerobes�
3. continued Given the opportunity, some species can proliferate and cause various pathology using a battery of exotoxins, some of which are the most potent toxins known to science.
Human pathogenic species include C. perfringens, C. tetani, C. botulinum, and C. difficile. As said before, C. difficile is unique among these species.
For the most part, penicillin is effective against Clostridial infections
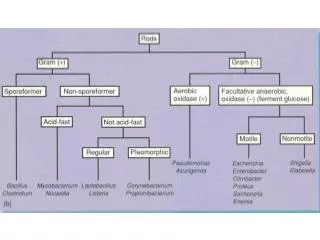
4. Clostridium � Presumptive ID Clostridia are obligately anaerobic endospore-forming Gram positive rods
Some have a tendency to easily over-decolorize, especially if a very young culture is not used for smear preparation.
Endospores may or may not be apparent on the Gram stain. Increasingly aerobic conditions prevent endospore formation in the Clostridia, whereas decreasing aerobiosis limits endospore production in Bacillus species. Confusion between these genera are not uncommon.
If endospores are not apparent the culture should be subjected to the heat-shock test or the ethanol tolerance test. Only endospore producers can withstand these adverse conditions
Wet-mounts may be superior to Gram stains to see endospores
5. Clostridium perfringens Text �C. perfringens is by far the most commonly isolated species from human sources.� But what about C. difficile? C. perfringens causes 2 primary conditions. One is a relatively mild but common food poisoning usually derived from meats, and causes S. aureus-like food poisoning symptoms.
The other is gas gangrene (ie. myonecrosis). �Gangrene� means death of tissue. Cells are introduced into flesh via traumatic implantation (historically a lot from war wounds) or surgical incision. Under anaerobic conditions they multiply, fermenting body substances producing gas & causing tissue disruption.
Mortality (often within 2 days) was high prior to better treatment including use of anti-toxin, surgical debridement, and widespread use of antibiotics (pennicillin). Death occurs via septic shock and numerous complications.
6. continued Lecithinase (alpha toxin) is the primary exotoxin: disrupts membranes and proteins = hemolysis and tissue necrosis, especially of muscle & connective tissue (vessels, etc). RBCs are disrupted = anemia, jaundice, and blood-tinged exudates. Gas pressure and disrupted tissues = crepitation (popping sounds) and compromised barriers. Amputation was common in war.
8. C. perfringens ID C. perfringens is the easiest Clostridium to speciate due to a unique combination of characteristics:
Anaerobic endospore-forming Gram positive rod (ID to Genus level)
Short fat square-ended rod with no apparent endospore in the Gram stain
Double zone hemolysis on SBA (only one in genus)
Positive reverse CAMP test with S. agalactiae (97% C. perfringens)
Lecithinase positive - Nagler test conducted using egg yolk agar with anti-lecithinase
�Stormy� fermentation in litmus milk due to acid and gas production
10. �reverse CAMP� result of C. perfringens (a, b & c)
11. Reverse CAMP Test
12. Nagler test: bottom half contains no anti-toxin therefore the opaque zone forms. Top half does contain the anti-toxin
13. Nagler Test
14. C. botulinum C. botulinum causes botulism, a rare but serious type of food poisoning. It has been historically associated with canned foods, either home canned or industrially. Other more commonly affected foods include home-cured ham, fermented fish, canned fruits (cranberries), and honey. A few recent cases involved native Alaskans eating whale meat.
The toxin, botulin or botulinum toxin, is the most potent toxin known. A mere trace is sufficient to cause paralysis and death. Like C. diptheriae, only C. botulinum cells lysogenized by a bacteriaphage can produce the toxin.
Botulin attaches to the neuromuscular junction of affected nerves preventing the release of acetylcholine causing �flaccid paralysis.� Death can occur within 2 hours due to smooth and/or cardiac muscle paralysis. Alternatively, symptom onset may not occur for a week.
15. continued Besides weakness and paralysis, double vision, impaired speech and difficulty in swallowing frequently occur
Infant botulism, unlike that in adults, follows ingestion of C. botulinum endospores, most commonly from honey. Lack of an established intestinal microbial community allows the organism to grow in the infant colon. Although rare, infant botulism is now the predominant type.
Fortunately, anti-toxin therapy results in complete recovery of all affected patients.
16. Flaccid paralysis from botulism
17. C. botulinum ID � Bailey & Scott C. botulinum is culturable, usually on AnBAP, but is not commonly cultured. Cells are usually seen in uneaten food.
Cells appear club shaped or raquet-shaped due to terminal swelling from sub-terminal endospores. Compared to C. tetani, diameter of swelling is greater in a plane parallel to the cell.
Spores may be evident in Gram stained smears or wet mounts.
Diagnosis via clinical presentation and demonstration of toxin in serum, stool or other GI sample, or in uneaten food
18. C. botulinum cells � note the evident terminal swelling from sub-terminal endospores
19. The BoTox alternative
20. C. tetani C. tetani causes tetanus, a rare (here & now) but frequently fatal neurological condition much like, but the opposite of botulism. The potent neruotoxin, tetanospasmin, inhibits release of neurotransmitters from neural synapse resulting in muscular rigidity via �spastic� paralysis. How exactly it does this is arguable. The Greek �tetanos� = �to stretch.�
As in botulism, skeletal muscles are affected first (one of the 1st is the maseter = trismus or �lockjaw�), but death results from smooth and/or cardiac muscle paralysis.
Infection results from introduction of spores, usually from the soil where they are common. One means of introduction is traumatic implantation, which is often occupationally related, or just working (or playing) around the yard. Rust has NOTHING to do with it, OK?
21. C. tetani Most cases worldwide are infants who contract the infection through the umbilical stump, either accidentally or from dung slapped on the umbilicus as part of a ritualistic ceremony
Most cases in the US (only 5/yr on avg) are in folks over 60 yrs age, maybe due to time since vaccination? Mortality rates run ~60% overall, and< 30% in the US.
Other symptoms include headache, difficulty swallowing, spasms, and sweating. Patients are extremely irritable.
Tetanus is the �T� in the DPT vaccine. It is a conjugated vaccine just like the other 2. A booster shot is required every ten years. The toxoid is the anti-toxin in this case.
22. tetanus
23. C. tetani ID C. tetani is culturable, usually on AnBAP, but is not commonly cultured. Cells are recoverable from wounds in ~1/3 of cases.
Cells are similar to those of C. botulinum but prevalence of cells with spores in a given smear may be more scarce. Spores are extreme terminal and appear bulbous with exaggerated swelling. Compared to C. botulinum, diameter of swelling is greater in a plane perpendicular to the cell.
Spores may be evident in Gram stained smears or wet mounts.
Diagnosis via clinical presentation and serology. Additional clinical evidence is generally absent and of little value.
24. C. Tetani � note the extreme terminal position of endospores and exagerated swelling
25. C. tetani colony on SBA
26. Clostridium difficle C. difficile is a common cause of diarrhea in hospitalized patients (it is nosocomial, fecal-oral) undergoing antimicrobial therapy (for > 4 days). Statistically, ~30% of hospitalized patients become infected and 1/3 of these develop diarrhea. It is also thought to be present in the colon of >30% of neonates. So C. perfringens is the most common Clostridia?
A complication of C. difficile diarrhea is a serious condition called antibiotic-associated pseudomembrane enterocolitis (PMC). Antibiotics kill off much of the normal gut flora giving this highly resistant organism an opportunity to proliferate.
C. difficile produces two potent toxins: an enterotoxin causing water loss and diarrhea (like cholera) and a cytotoxin causing pseudomembrane formation
27. Clostridium difficle Therapy includes discontinuation of the original antibiotic (often ampicillin) allowing the gut flora to re-establish and out-compete the pathogen. Severe cases require use of vancomycin.
Reported mortality rates (10-30%) are exaggerated by the compromised status of the host.
C. difficile can be isolated on a selective agar medium (Cycloserine-Cefoxitin-Fructose Agar or CCFA), but this is generally not recommended because C.difficle can be isolated from healthy people and not all strains isolated are toxigenic
Diagnosis is by clinical presentation and by serological confirmation of the toxins. An ELISA test is available.
28. Identification of Clostridium
29. Presumptive Identification