Download
1 / 91
920 likes | 1.35k Vues
Bacilus Anthracis Anthrax. Sheref Hassan Rachel Handwerger Maria Garrido. “The Agent”. CDC: Category “A” Biological Agent Vegetative cell: large, gram-positive bacillus ( 1.0-1.5 μ m by 3.0-5.0 μ m)

E N D
Bacilus AnthracisAnthrax Sheref Hassan Rachel Handwerger Maria Garrido
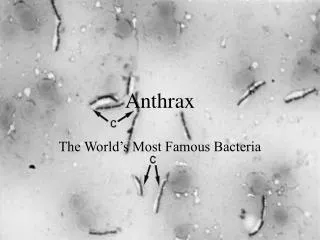
“The Agent” • CDC: Category “A” Biological Agent • Vegetative cell: large, gram-positive bacillus (1.0-1.5 μm by 3.0-5.0 μm) • Endospore: oval, central-to-sub terminal, does not usually swell (1.0x1.5 μm);CO2 levels within the body inhibit sporulation • Forms long chains in vitro; forms single cells or short chains in clinical samples • Aerobic or facultative anaerobic; non-motile; catalase-positive • Nonhemolytic on sheep blood agar; susceptible to lysis by gamma phage • Colonies: ground-glass appearance and consistency of beaten-egg whites and are 2-5 mm in diameter after 16-18 hours of incubation
“The Agent” contd.. • In environments rich in nutrients such as glucose, amino acids, and nucleosides, spores will germinate and form vegetative cells. Vegetative bacteria survive poorly outside of mammalian host. • In a nutrient-deficient setting, vegetative cells will form spores. • *Spores have been shown to survive in the environment for more than 40 years.
History of Anthrax:Early History • The first recorded report of anthrax was during the fifth Egyptian Plague in 1500 B.C. responsible for the death of a large amount of livestock. • The sixth Egyptian Plague, also known as the “plague of boils” was probably the first recorded instance of cutaneous anthrax and was responsible for many deaths. • The “Black Bane” in Europe during the 1600s killed well over 60,000 cattle and typified anthrax symptoms. • 1863: French biologist Casimir-Joseph Davaine makes B.A. the first microorganism to be conculsively linked to a disease. • 1876: B.A. isolated in pure culture for the first time by Robert Koch • Was also called: wool sorter’s disease, Bradford disease, and rag picker’s disease.
History of Anthrax:Early History • 1897: The Bradford Rules are passed as law Anthrax Investigation Board. • 1919: The Anthrax Prevention Act passed in England established a wool-disinfecting complex in Liverpool. • Similar laws, gov’t regulations, better disinfectant methods and technology thereafter reduced Anthrax cases linked to occupational hazards, as well as making Anthrax viability and outbreaks rare in the modern world.
History of Anthrax:Natural Outbreaks Animal: • 1945: Iran outbreak causes 1 million sheep deaths
History of Anthrax:Natural Outbreaks - cont... Inhalation: • U.S. 1900-1978: only 18 reported cases mostly among high risk groups such as goat mill or goatskin workers and wool or tannery workers (only 2 were laboratory associated) • New Hampshire 1957: 5 cases reported in goat-hair processing plant • No Case of inhalation anthrax was reported since 1978 in the U.S. prior to post-Sept. 11th attacks.
History of Anthrax:Natural Outbreaks - cont... Cutaneous (most common): • U.S. 1944 -1994: 224 cases reported • New Hampshire 1957: 4 cases reported in goat-hair processing plant • Zimbabwe 1979-1985: largest reported epidemic with over 10,000 reported human cases and 182 deaths (nearly all cutaneous); explained by spread via insect vectors or contaminated meat; however, biological warfare tactics have been also postulated
History of Anthrax:Natural Outbreaks - cont... Gastrointestinal (uncommonly reported): 2 distinct syndromes: oral pharyngeal (unusual manifestation of infection and is of more interest)& abdominal disease • Since mid 1970’s: small outbreaks reported in Africa and Asia • Northern Thailand • 1982: 24 cases of oral pharyngeal reported due to the consumption of contaminated buffalo meat • 1987: 14 cases involving both oral pharyngeal and abdominal disease
Statistics of Anthrax Occurrences In the U.S.: • Approximately 130 cases occurred annually in the early 1900’s • This number decreased with less than 10 cases reported each year since the early 1960’s and no occurrences from 1978 until after Sept. 11th 2001 • 95% of naturally occurring cases are cutaneous and 5% are due to inhalation. (cases of gastrointestinal anthrax have not been recognized yet in the U.S.) • Only 18 cases of naturally occurring inhalation cases have been reported during the 20th century with the most recent in 1976 • Since 1990, only 2 cases (1992 and 2000) of naturally occurring infection have been reported (both cutaneous).
Statistics of Anthrax Occurrences Globally: • Approximately 2,000 - 20,000 cases of anthrax occur each year. • Most cases are cutaneous with inhalation and gastrointestinal being less frequent. • Human cases usually follow disease occurrences in ruminants and are most prevalent in Africa, the Middle East, and parts of Southeast Asia.
“Travelers Beware” Anthrax in animals is hyper-endemic or endemic in: (caution when eating meat in these areas) • Most areas of the Middle East • Most areas of equatorial Africa • Mexico and Central America • Chile, Argentina, Peru, Bolivia • Certain Southeast Asian countries such as Myanam, Vietnam, Cambodia, & Thailand • Papua New Guinea • China • Some Mediterranean Countries (for more information see WHOCC)
A B A1 A2 A3 A4 B1 B2 Bacillus anthracis • Review: • Gram Positive • Rod shaped • Aerobic • Spore Forming • Non-motile
Bacillus anthracis Bacillus anthracis exists in two forms: • Inert spore form • 1 μm • Rod shaped • Aerobic (free O2 present) • Highly Resistant to extreme conditions (e.g. temperature, weather, radiation, etc.) • Spores have been known to last up to 40 yrs
Bacillus anthracis • Vegetative form • 1 – 1.5 μm by 5 – 8 μm • Square-ended rod • Anaerobic environment of host • Only multiply within host in the presence of amino acids, nucleosides, and glucose
Bacillus anthracis • Bacillus anthracis is composed of: • A capsule • A three part protein • Protective Antigen (PA) • Edema Factor (EF) • Lethal Factor (LF) • In the bacteria there is one chromosome and 2 plasmids (pXO1 and pXO2)
Bacillus anthracis • Chromosome not involved in virulence • pXO1 codes for PA, EF, and LF • pXO2 codes for the capsule
pXO2/Capsule • pXO2 codes for the homopolymeric -linked poly-D-glutamic acid capsule • Contains three genes: capBCA • 96,231 bp, ~85 ORFs (16 sm. ones) • Antiphagocytic function • Is non-toxic by itself • Is important in the onset of the infection • Poorly understood
pXO1 • 181,654 nucleotides, ~143 ORFs • Codes for the three toxin genes which are transcribed simultaneously: • pagA (for PA) • cya (for EF) • lef (for LF) • Codes for regulatory proteins, from the atxA gene, which causes ~10x increase in transcription of all three toxins
PA • Is non-toxic without EF and LF • Coded from pag gene • A/T rich (69%) • Cysteine-free • 83 kDa (735-amino acid) • Long, flat protein • Function – to aid in the insertion of EF and LF toxins in the cytosol
PA Structure • Domain 1 (Green and Blue) • residues 1 – 249, β-sandwich fold, • 2 Ca2+, forms cleavage site during proteolytic activation • Domain 2 (Magenta) • Residues 250 – 487, β-barrel core • Forms membrane inserted channel /pore formation • Domain 3 (Yellow) • Residues 488 – 594, 4-stranded mixed β-sheet, 4 small helices • Helps to oligomerize(?) • Domain 4 (Purple) • Residues 595 – 735, β-sandwich • Contains receptor binding domain Koehler, T.M. Anthrax. Springer. 2002.
PA Mechanism • Mechanism: • PA83 binds to cell receptor • Furin or a furin-like molecule cleaves PA83 between aa 164-167 (Arg-Lys-Lys-Arg) to two fragments: PA20 (released) and PA63 (remains attached to the receptor) http://www.biotechjournal.com/Pathways/anthrax.htm
PA Mechanism (cont.) • PA63/receptor complexes join to form a heptamer at reduced pH • The heptamer complex can then bind to one LF or EF molecule at each subunit http://www.biotechjournal.com/Pathways/anthrax.htm
PA Mechanism (cont.) • The heptamer is internalized via RME • Acidification of the vesicle causes the heptamer to form a pore in the membrane • EF and LF are released through the pore into the cytosol Koehler, T.M. Anthrax. Springer. 2002.
General Mechanism Koehler, T.M. Anthrax. Springer. 2002.
EF • Coded from cya gene • A/T rich (71%) • Cysteine-free • 89 kDa (767-amino acid) • Mainly β strands • N-terminal ~250 aa bind to PA63 • Remaining molecule possesses catalytic activity in substrate and calmodulin-binding subdomains • A-B toxin
EF Function • EF receptors are present on most cells • EF is a calmodulin dependent adenylate cyclase • Therefore only functions in eukaryotic cells • Catalyzes breakdown of ATP to cAMP • ~200 fold increase • Why Calmodulin? • 1% total cellular protein • Responsible for mediating Ca2+ signaling in cells
EF Mechanism • Mechanism • EF enters the cell by binding to PA (called EdTx) • Inside, EF binds to calmodulin at the N-terminal low Ca2+ affinity site in a very unique way: • One half grips lower lobe while the other grasps the upper lobe and twists • The method of binding forms a contact region of 6,000 Å2 – an extremely large binding region! • The conformational change experienced by both molecules inhibits Ca2+ from binding and inhibits the reverse reaction of cAMP to ATP
EF Mechanism (cont.) • The conformational change in EF allows it to act as an adenylate cyclase and bind to ATP • cAMP is formed due to the binding of EF to ATP Liddington, R.C., A Molecular Full Nelson. Nature. 415: 373-374, 2002.
EF • What happens as a result of this activity? • Causes edema by altering H2O and ion movement • Inhibits immune response against Bacillus anthracis http://www.biocarta.com/pathfiles/h_anthraxPathway.asp
EF • Inhibits activity of TF NF-ĸB in macrophages • Strains with only EF and PA (LF-) are not likely to be lethal
LF • Coded from lef gene • A/T rich (70%) • Cystenine-free • 90.2-kDa (776-amino acid) • 3 domains: • N-terminal ~250 aa competes with EF to bind PA63 • 5 imperfect repeats, each 19 aa long • Contains a zinc protease active site (HEXXH helix) • A-B Toxin Pannifer, A.D., Wong, T.Y., et al, Crystal Structure of the Anthrax Lethal Factor. Nature. 414: 229-233, 2001.
LF Function • LF only binds to macrophages • LF is responsible for most of the toxicity • Can induce lysis in about 90-120 minutes • LF is a zinc dependent metalloprotease which cleaves MAPKK
LF Mechanism and Function • LF is internalized via PA (called LeTx) • Mechanism and Result of MAPKK cleavage: • LF cleaves between 7-10 residues on the N-terminus of the MAPKKs at a pair of proline residues (separtated by 0 – 4 aa) • E.g. MAPKK1, 2, 3, 4, 6 Duesbery, N.S., Vande Woude, G.F., Anthrax Toxins. Cellular and Molecular Life Sciences. 55: 1599-1609, 1999.
LF Mechanism and Func. (cont) • This cleavage serves to inactivate the MAPKK • MAPKK cleavage leads to lysis of the macrophages, although the mechanism is unclear http://www.biotechjournal.com/Pathways/anthrax.htm
LF Mechanism and Func. (cont) • Some MAPKK aid in the activation of TF NF-ĸB • This illustrates how EF and LF work together to promote macrophage lysis
LF Mechanism and Func. (cont) • At sublytic levels it stimulates production of IL-1β and TNFα • At lytic levels the mechanism is unclear, but it is possible that in the early stages they inhibit the immune response to allow the bacteria to proliferate, and at later stages it stimulates them to cause lysis of cells • Causes leakage in cell membrane without ATP increased Ca2+ conc. in cell • Strains with only LF and PA (EF-) are likely to be lethal, although to a lesser degree
EF Increased production of cAMP Causes swelling Inhibits immune response Allows for invasion! LF Cleaves MAPKKs Inhibits immune response Destroys macrophages Cells can’t fight off infection they Die! Review
Overall Mechanism Review Duesbery, N.S., Vande Woude, G.F., Anthrax Toxins. Cellular and Molecular Life Sciences. 55: 1599-1609, 1999.
Clinical Features of B. Anthracis • Anthrax can manifest itself in 3 forms: cutaneous, gastrointestinal, & inhalational (pulmonary). • The type contracted depends on the modes of transmission, which include: • Contact with infected tissues of dead animals (eg, butchering, preparing contaminated meat) cutaneous • Consumption of contaminated undercooked meat gastrointestinal • Contact with contaminated hair, wool, or hides (during processing) or contact with products made from them inhalational &/or gastrointestinal • biological warfare mainly inhalational &/or gastrointestinal
Pathology Inhalational Anthrax: • Endospores are introduced into the body and alveoli via inhalation. (small size of spores permits this) • Macrophages phagocytose and lyse endospores, and then travel to regional lymph nodes. • Spores germinate to become vegetative cells within macrophages; they then leave macrophages and multiply within the lymphatic system. (1-43 days) • Bacteria enter the bloodstream and can lead to septic shock and toxemia with system wide edema and necrosis; hematogenous spread can lead to hemorrhagic meningitis. • True pneumonia is rare w/ inhalational anthrax but focal, hemorrhagic, necrotizing pneumonic lesions may be observed. • Major causes of death is compression of lungs and septic shock.
Pathology cont… Inhalational Anthrax: • Development of symptoms and pathogenesis occurs in 2 stages: • Exhibition of cold and flu like symptoms malaise, fever, prominent cough, nausea, vomiting, drenching sweats, dyspnea, chest pain, and headaches • Develops rapidly (hours) and is characterized by acute dyspnea, subsequent cyanosis, pleural effusion, widened mediastinum, pulmonary edema, hemorrhagic symptoms of stage 1 become severe (>24hrs and leads to death) • ID50 (infective dosage that will infect 50% of exposed) is 8,000-50,000 spores. • LD50 (Lethal dosage that will kill 50% of exposed) is 2,500-55,000 spores. • Untreated 80% mortality rate
Pathology cont… Cutaneous Anthrax: • Endospores enter body through the skin usually via preexisting skin lesions, abrasions, and skin mucus membranes. • Low-level germination and toxin production occurs at entrance site leading to localized necrosis with eschar formation and edema (massive in some cases) • Eschar formation: • Day 1 pruritic red papule appears at the initial site of infection • Day 2 papule becomes round ulcer • Day 3 plaque develops around edema site and central papule necrotizes, ulcerates, and forms a normally painless black eschar • After 1-2 weeks eschar falls off and leaves ulcer that can heal by week 3.
Pathology cont… Anthrax eschar, neck CDC Public Health Image Library, number 1933 Anthrax eschar, neck CDC Public Health Image Library, number 1934 Edema around anthrax lesion AB Christie, Liverpool
Pathology cont… Cutaneous Anthrax: • Endospores are often phagocytosed by macrophages and carried to local lymph nodes, which can result in painful lymphadenopathy and lymphangitis • Hematogenous spread with resultant toxemia can occur, with symptoms such as headache and fevers (up to 102 °F) although such spread is not common with appropriate antibiotic therapy • On very rare occasions system wide infection can occur and results in death within days. • ID50 & LD50 are unknown for cutaneous anthrax • Untreated mortality rate is 20% • With antibiotic treatment death is very rare.
Pathology cont… Gastrointestinal Anthrax: • Pathogenesis and statistics are unclear due to rarity of this form • Vegetative cells from uncooked meat rather than spores (germination unnecessary) • In oral pharyngeal anthrax, bacteria enter via the oral or pharyngeal mucosa mucosal ulcers can occur initially, followed by local/regional lymphadenopathy and localized edema. • In abdominal anthrax, entrance occurs @ the ileum or cecum Intestinal lesions, regional lymphadenopathy, and edema of the bowel wall and ascites initially causes nausea, vomiting, and malaise progressing into bloody diarrhea, acute abdomen, or sepsis. • Mortality may drop with antibiotic treatment (inconclusive)
Diagnosis • Because of rarity of gastrointestinal cases diagnosis focus is limited. Onset of characteristic symptoms should signal patient to consult a physician immediately for antibiotic treatment. • Cutaneous anthrax can be distinguished by 2 key features: painlessness of lesions and relatively large extent of associated edema (presence of eschars) • Distinguishing features of inhalational anthrax: presence of widened mediastinum and pleural effusions on chest radiograph or CT (chest compound tomographic) scan with minimum evidence of pneumonia.
Diagnosis cont… Pulmonary anthrax chest X-rayshowing widened mediastinum Dept of Radiological PathologyArmed Forces Institute of Pathology Inhalational Anthrax: • Easier to diagnose when occurs in several suspicious cases than single case (or at high risk situations postal employee) • chest x-ray showing a widened mediastinum, infiltrates, pleural effusion, etc. = likely anthrax infection • CT scan showing hyperdense hilar and mediastinal nodes (white arrow, middle diagram) + extensive mediastinal edema = anthrax infection • Molecular Biology tests only available at Laboratory Response Network (LRN) labs but highly reliable
Diagnosis cont… Distinguish Anthrax from Influenza-Like Illness (ILI): • Early symptoms (fever, chills, myalgias, fatigue, malaise, and nonproductive cough) are similar. • ILI patients have rhinorrhea and this is uncommon in Anthrax patients. • Anthrax patients have shortness of breath, an uncommon trait of ILI patients. • Nausea and vomiting are more common in anthrax infection • Abnormal chest radiographs and CT scans Anthrax infection