Download
1 / 34
440 likes | 1.2k Vues
Non Hodgkins Lymphoma. M. Mahmood Khan, MD Hematology-Oncology 12/5/03. Lymphomas . Tumors of The Lymphoid Tissue 4% of all cancers Mostly ‘solid’ tumors … but may occasionally have an additional leukemic component !. Simplified schema of Hematopoetic Cancers. WBC.

E N D
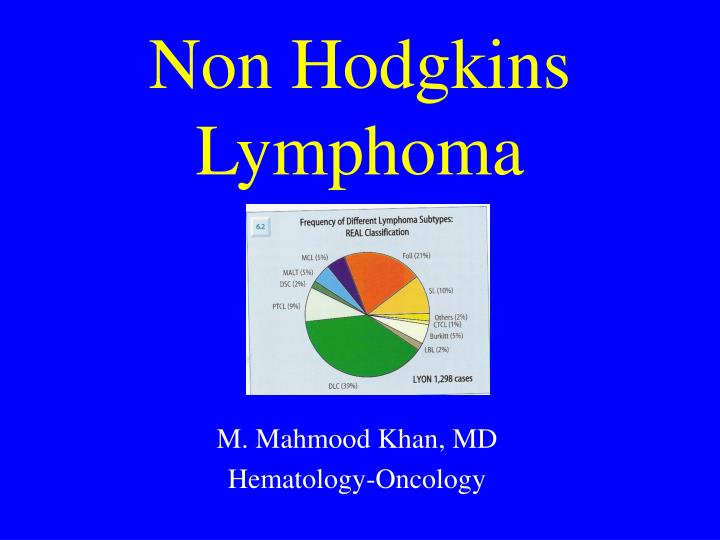
Non HodgkinsLymphoma M. Mahmood Khan, MD Hematology-Oncology 12/5/03
Lymphomas • Tumors of The Lymphoid Tissue • 4% of all cancers • Mostly ‘solid’ tumors … but may occasionally have an additional leukemic component !
Simplified schema of Hematopoetic Cancers WBC Acute and chronic Myeloid ‘Leukemias’ RBC Myeloid Platelets Hematopoetic Stem Cell B Cells Lymphomas Hodgkins (30%) Non Hodgkins (70%) Lymphoid T cells
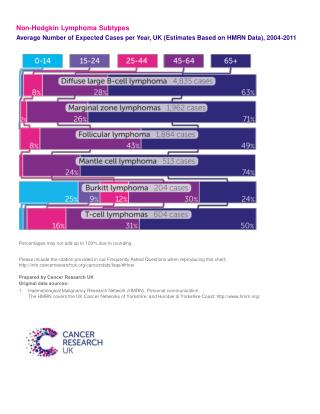
NHL: Incidence • 56,000 cases /year. • 25,000 deaths per year • Incidence rose 1973- 1998 • Better diagnosis, aging population and HIV • 4% of all cancers • 85% are B cell type and 15% are T cell type
NHL: Etiol. & Pathogenesis (contd). • Viruses: HTLV 1 : associated with Adult T cell Leukemia/Lymphoma EBV : Burkitts Lymphoma, esp in endemic form (95%), PTLD, some AIDS associated NHL and all AIDS associated primary CNS lymphoma HHV8 : Kaposi’s Sarcoma and primary effusion lymphoma • Helicobacter Pylori:MALT lymphoma
NHL : Pathogenesis (contd). Chromosomal translocations • t(8:14) seen in Burkitts Lymphoma • t(14:18) >80% of follicular NHL, leads to over expression of ‘anti apoptotic gene’ bcl-2 • t(11:14) seen in almost all Mantle Cell lymphomas
NHL: Etiology and PathogenesisEnvironmental Factors • Inconsistent and contradictory studies • Higher risk associated with several occupations: Farmers, agricultural workers chemists • Causal relationship not established
NHL: Classification(s) • Lukes and Collins (1970s) • NCI working formulation (1980s) • R.E.A.L Classification: Revised European American Classification (1990s) • WHO classification, 2000
NHL Classification (contd). NCI WORKING FORMULATION • Clinically very useful and practical • Divides lymphomas into : 1. Low grade 2. Intermediate grade and 3. High grade NHL • Based on morphology (Architecture and Cell size) • Examples: DiffuseLarge cell NHL Follicularsmall cell NHL
NHL : Classification (contd). • Low grade /Indolent NHL Are INCURABLE • Intermediate /High Grade Are more “Aggressive” but potentially CURABLE!
B Cell Neoplasms Precursor B Cell Neoplasms: Lymphoblastic Lymphoma/ALL Mature B Cell Neoplasms: CLL/SLL MALT Diffuse Lg B Cell Mantle Cell Burkitts Lymphoma/Leukemia Plasma cell Myeloma Uncertain Malignant Potential: PostTransplant Lymphoprolif.dis T Cell and NK Cell Precursor T cell Neoplasms Lymphoblastic lymphoma/Leukemia Mature T Cell Neoplasms Primary T cell lymphoma (NOS) Angio immuno blastic lymphoma Mycosis Fungoides/Sezary Anaplastic LCL,primary systemic type NHL : WHO Classification(most common subtypes)
NHL : Clinical Presentation • Indolent types: Present typically at advanced stage, with L.N., spleen or marrow disease • Aggressive NHL: Present as enlarging mass in nodal, or extra nodal areas. H&N, liver, GI, skin, marrow and bone are more common extra nodal sites. • Lymphadenopathy in NHL is typically non tender, firm or rubbery • ‘B’ symptoms : Fever, drenching nite sweats or Wt. Loss >10% in 6 months
H & P CBC, Chemistry, LDH Excisional LN biopsy, also send for immunophenotyping (flow cytometry) and cytogenetics NHL : Diagnosis and Staging procedures
NHL: Diagnosis & Staging procedures (contd). • CT scan of chest, abdomen and pelvis • PET scan • Bone Marrow Biopsy • Lumbar Puncture if CNS symptoms or aggressive lymphoma with bone marrow involvement
Stages of NHL Ann Arbor Staging System • I : 1 L.N. site (or one extra nodal site, IE) • II : 2 or more L.N. sites (same side of diaphragm) • III: Involvement above and below diaphragm • IV: Diffuse or disseminated involvement of 1 or more extralymphatic tissues or organs • (A= Absence of systemic symptoms, B= Presence of B symptoms)
HD: Ann Arbor Staging Sytem I II III I IV
NHL: Ann Arbor Staging System • Suffix ‘A’ means absence of B symptoms • Suffix ‘B’ means presence of B symptoms • Suffix ‘E’ means extra nodal disease • Suffix ‘S’ means splenic involvement • Suffix ‘X’ means bulky disease • For example: Stage IIIB-S means disease above and below the diaphragm, with B symptoms and Splenic involvement
NHL: Two Commonest subtypes • Diffuse Large Cell Lymphoma • Follicular Lymphoma
NHL : Diffuse large cell Lymphoma • Commonest subtype • Classified as ‘intermediate grade’ in WF • Heterogenous disease 40% are cured with standard CHOP therapy 40% respond initially but later relapse 20% are refractory to any therapy IPI : International Prognostic Index is used to estimate prognosis in an individual patient
5 ‘risk factors’ should be identified in each pt. At the time of diagnosis 1) Age >60 2) LDH> normal 3)ECOG performance status 2-4 Stage III or IV Two or more extranodal sites Score/risk category 5 yr survival Score 0-1= low risk 73% Score 2 = Low Intermed 51% Score 3 = High Intermed 43% Score 4-5= High risk 26% (Shipp et al Blood 1994:83:1165) Diffuse Large Cell NHLInternational Prognostic Index
Therapy: Diffuse Large Cell Lymphoma • Limited stage (I or II) Non bulky: Combination of abbreviated chemotherapy (3-4 cycles of CHOP) and radiation • Advanced Stage (III or IV) or bulky disease: Full 6-8 cycles of chemoRx with additional XRT to bulky areas • Chemotherapy regimen is CHOP: Cyclophosphamide, Hydroxydoxorubicin, Oncovin and Prednisone)
‘CHOP’Chemotherapy • CHOP regimen was developed >20 years ago! • Several attempts to improve upon its efficacy by adding drugs or increasing dose failed
1138 pt, intergroup trial Randomized comparison of CHOP vs more intensive regimens: - m-BACOD - ProMACE-cytaBOM - MACOP-B Results: CHOP was as good as others and was less toxic (Fisher RI, NewEng J Med 1993,328:1002) Large Cell NHL/ Rx:Improving upon ‘CHOP’
French group ‘GELA’ Randomized trial 399 pts Elderly (higher risk pts) CHOP x 8 +/- Rituximab Improved results with addition of ‘Rituxaimab’ RR 63% 75% 2yr EFS 38%57% 2 yr OS 57%70% (Coiffier B; N Eng J Med 2002:346:235) NHL Rx: Improving upon ‘CHOP’(adding Rituximab)
Randomized trial (PARMA) n = 109 ‘Chemosensitive relapses’ Std.salvage chemo vs Hi dose chemo stem cell transplant Better 5yr EFS(46% vs 12%) Better 5 yr OS (53% vs 32%) Based on this study High dose chemotherapy followed by Autologous SCT has become the standard of care in relapsed large cell lymphoma. Large Cell NHLRX of Relapsed disease
Monoclonal anti CD 20 antibody CD 20 is a cell surface receptor present on all B lymphocytes Rituximab (Rituxan) binds to CD 20 and eventually leads to cell lysis Very well tolerated drug, infusion reactions are possible NHL Therapy: RITUXIMABTargeted therapy or Immunotherapy
Conjugating Radio isotopes to anti CD 20 Antibody has further enhaunces its activity Myelosupression Secondary Myelodysplasia NHL Targeted Therapy:Radioimmunotherapy (Ibritumomab-Y90)
INDOLENT LYMPHOMASFollicular Lymphoma • Typically presents as advanced stage • Some patients are asymptomatic at diagnosis • This disease is incurable so far • Watchful waiting is acceptable in asymptomatic patients • Therapy is required for disease related symptoms
Indolent lymphomasFollicular NHL • Single agent oral ‘Chlorambucil’ is useful therapy esp in elderly patients • More aggressive regimens: CVP, CHOP or Fludarabine. • Multi drug combinations improve response rate but does not result in cure • Rituximab has become an extremely useful drug in these paitents. • Radioimmunotherapy is also useful. • High dose chemotherapy and transplantation has not resulted in cure so far. Area of active research.
Other ImportantNon Hodgkins Lymphomas • Mantle Cell Lymphoma: Extremely challenging disease, CHOP-R results in remissions but never cure, consider early transplantation. • Gastric MALT Lymphoma: Represents exaggerated immunologic response to H Pylori. Initial therapy should be directed against Helicobacter Pylori (Flagyl,Amoxicillin,Omeprazole). 70% patients respond! • Small Lymphocytic lymphoma and Chronic Lymphocytic Leukemia: are ‘one and same’ disease. SLL is lymph node based and CLL is leukemic. Rx and prognoses are same
ConclusionsNON HODGKINS LYMPHOMA • Extremely heterogenous group of disease • WHO classification is probably going to stay • Indolent NHL : Slow growing but incurable • Aggressive NHL: Faster growing but/therefore potentially curable • Follicular NHL: Commonest indolent type • DLCL: Commonest aggressive type • Intl.Prog.Index (IPI): Valuable predictor of outcome in an individual patient