Download
1 / 68
1.43k likes | 4.49k Vues
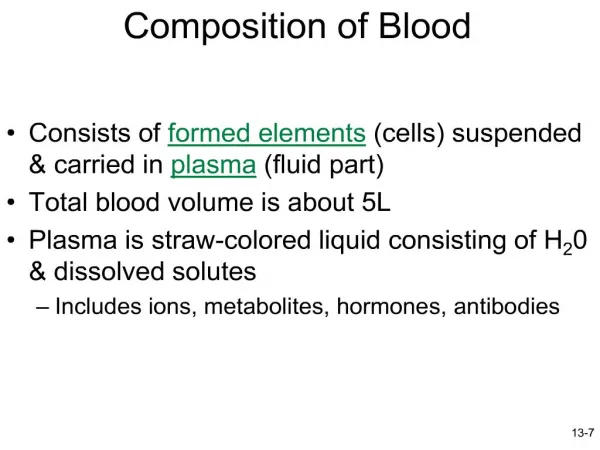
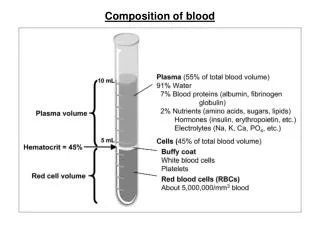
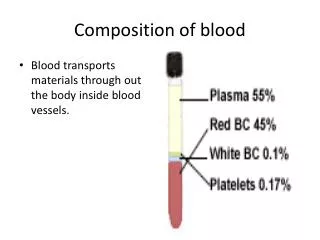
Composition of Blood. Blood is the body’s only fluid tissue It is composed of liquid plasma and formed elements Formed elements include: Erythrocytes, or red blood cells (RBCs) Leukocytes, or white blood cells (WBCs) Platelets

E N D
Composition of Blood • Blood is the body’s only fluid tissue • It is composed of liquid plasma and formed elements • Formed elements include: • Erythrocytes, or red blood cells (RBCs) • Leukocytes, or white blood cells (WBCs) • Platelets • Hematocrit – the percentage of RBCs out of the total blood volume
Components of Whole Blood Figure 17.1
Physical Characteristics and Volume • Color varies from scarlet to dark red • The pH of blood is 7.35–7.45 • Temperature is 38C (100.4 F) • Blood accounts for approximately 8% of body weight • Blood Viscosity 4.5 – 5.5 centipoise per second • Average volume: 5–6 L for males, and 4–5 L for females • Isotonic with a 0.9% NaCl solution • Osmolarity 276 – 295 milliosmoles per Kg
Formed Elements • Erythrocytes, leukocytes, and platelets make up the formed elements • Only WBCs are complete cells • RBCs have no nuclei or organelles, and platelets are just cell fragments • Most formed elements survive in the bloodstream for only a few days • Most blood cells do not divide but are renewed by cells in bone marrow
Leukocytes (WBCs) • Leukocytes, the only blood components that are complete cells: • Are less numerous than RBCs • Make up 1% of the total blood volume • Can leave capillaries via diapedesis • Move through tissue spaces • Leukocytosis – WBC count over 11,000 / mm3 • Normal response to bacterial or viral invasion
Groupings of White Blood Cells • White blood cells are divided into the Granulocytes and Agranulocytes. • A granule is a stained vesicle. A vesicle is a membrane bound organelle in a cell that contains certain chemicals. • Cells are translucent so in order to see them adequately under the microscope a chemical stained is placed on the cells. The chemical stain binds chemically to chemicals in the cell – thus when the slide is rinsed with water the stain remains – giving a certain color to cellular components for identification purposes.
Peripheral Smear & Staining (1) • In order to look at blood under the microscope – a peripheral smear is made. The term means to take blood from the peripheral blood vessels (those not in the bone marrow) and place a drop of it on a slide and smear it. Since cells are translucent – a stain must be used to see the blood cells for the purpose of identification. • So the first order of business is to do a finger stick or some other method to get a very small amount of blood.
Peripheral Smear & Staining (2) • A droplet of blood is then placed at the corner of a microscope slide. • A second microscope slide is then used to push the blood into a very, very thin smear. Note – you do not want cells stacked on top of one another because you cannot see the blood cell underneath for ID purposes.
Peripheral Smear & Staining (3) • Next a chemical stain is placed on the slide of smeared blood. A chemical stain is a chemical (in some cases a mixture of chemicals) in which the chemicals have certain colors (dye) that chemically bond to certain chemical components of a cell. Since the chemicals bond to the chemical components of the cell – they will not wash off when the slide is flooded (rinsed) with water. • For blood the current staining method uses a stain derived from Romanovsky in the 19th century. This stain is a combination of Methylene Blue and Eosin. Modifications of these stains (change in the percentage of the two chemicals) produced the Wright Stain and Giemsa stain – which are the two staining chemicals used to stain blood in most labs – including the one here at Kingwood. • Methylene blue has a blue color and is a chemical base (pH) thus it stains acidic components of a cell. • Eosin is red and is an acid – thus it stains basic components of a cell. • Some components of a cell color a reddish blue by binding to azures, substances formed when methylene blue is oxidized.
Peripheral Smear & Staining (4) • Now the non-stained blood slide is then flooded with stain. It sits for a few moments – then the slide is flooded with water to wash off the non-chemically bound stain. As you know nothing is perfect so some stain may not wash off – and form artifact on the slide.
All of the white blood cells have vesicles but the granulocytes have more vesicles than the agranulocytes. Thus the accepted term agranulocyte is really misleading. The agranulocytes have only primary vesicles (granules) which are the cell’s stained lysosomes. The granulocytes have the primary granules plus secondary vesicles (granules). The secondary granules are special chemicals unique to each of the granulocytes – thus they are termed “specific granules” . It is the chemicals in the secondary vesicles (granules) that determine each granulocytes function.
The Granulocytes are the neutrophils, eosinophils and the basophils • The Agranulocytes are the lymphocytes and monocytes
Percentages of Leukocytes Figure 17.9
Granulocytes • Granulocytes – neutrophils, eosinophils, and basophils • Contain secondary cytoplasmic granules that stain specifically (acidic, basic, or both) with Wright’s stain • Are larger and usually shorter-lived than RBCs • Have lobed nuclei
Neutrophils also known as Polymorphonuclear Leukocytes (PMNs) • Neutrophils have two types of granules that: • Take up both acidic and basic dyes • Give the cytoplasm a lilac color • Contain peroxidases, hydrolytic enzymes, and defensins (antibiotic-like proteins) • Neutrophils are our body’s bacteria slayers Nucleus has 3 – 6 lobes
Eosinophils • Eosinophils account for 1–4% of WBCs • Have red-staining, bilobed nuclei connected via a broad band of nuclear material • Have red to crimson (acidophilic) large, coarse, lysosome-like granules • Lead the body’s counterattack against parasitic worms • Lessen the severity of allergies by phagocytizing immune complexes and produce an antihistamine
Basophils • Account for 0.5% of WBCs and: • Have U- or S-shaped nuclei with two or three conspicuous constrictions • Are functionally similar to mast cells • Have large, purplish-black (basophilic) granules that contain histamine & heparin • Histamine – inflammatory chemical that acts as a vasodilator and attracts other WBCs (antihistamines counter this effect)
Agranulocytes • Agranulocytes – lymphocytes and monocytes: • Lack visible cytoplasmic granules • Are similar structurally, but are functionally distinct and unrelated cell types • Have spherical (lymphocytes) or kidney-shaped (monocytes) nuclei
Lymphocytes • Account for 25% or more of WBCs and: • Have large, dark-purple, circular nuclei with a thin rim of blue cytoplasm • Are found mostly enmeshed in lymphoid tissue (some circulate in the blood) • There are three types of lymphocytes: T cells, B cells and natural killer cells (NK cells) – however only the T & B lymphocytes circulate in the blood • T cells function in the immune response • B cells give rise to plasma cells, which produce antibodies
Monocytes • Monocytes account for 4–8% of leukocytes • They are the largest leukocytes • They have abundant pale-blue cytoplasms • They have purple-staining, U- or kidney-shaped nuclei • They leave the circulation, enter tissue, and differentiate into macrophages
Leukocytes Figure 17.10
Summary of Formed Elements Table 17.2.1
Summary of Formed Elements Table 17.2.2
Formation of Leukocytes • All leukocytes originate from hemocytoblasts • Hemocytoblasts differentiate into myeloid stem cells and lymphoid stem cells • Myeloid stem cells become myeloblasts or monoblasts • Lymphoid stem cells become lymphoblasts • Myeloblasts develop into eosinophils, neutrophils, and basophils • Monoblasts develop into monocytes • Lymphoblasts develop into lymphocytes
Stem cells Hemocytoblast Myeloid stem cell Lymphoid stem cell Committed cells Myeloblast Myeloblast Myeloblast Lymphoblast Develop- mental pathway Promyelocyte Promyelocyte Promyelocyte Promonocyte Prolymphocyte Eosinophilic myelocyte Basophilic myelocyte Neutrophilic myelocyte Eosinophilic band cells Neutrophilic band cells Basophilic band cells Monocytes Lymphocytes Eosinophils Basophils Neutrophils (a) (b) (c) (e) (d) Some become Agranular leukocytes Granular leukocytes Some become Macrophages (tissues) Plasma cells Figure 17.11
Platelets • Platelets are fragments of megakaryocytes with a blue-staining outer region and a purple granular center • Their granules contain serotonin, Ca2+, enzymes, ADP, and platelet-derived growth factor (PDGF) • Platelets function in the clotting mechanism by forming a temporary plug that helps seal breaks in blood vessels • Platelets not involved in clotting are kept inactive by NO and prostacyclin
Genesis of Platelets • The stem cell for platelets is the hemocytoblast • The sequential developmental pathway is as shown. Stem cell Developmental pathway Hemocytoblast Megakaryoblast Promegakaryocyte Megakaryocyte Platelets Figure 17.12
SamplesA phlebotomist collects the specimen, in this case blood is drawn in a test tube containing an anticoagulant (EDTA, sometimes citrate) to stop it from clotting, and transported to a laboratory.In the past, counting the cells in a patient's blood was performed manually, by viewing a slide prepared with a sample of the patient's blood under a microscope (a blood film, or peripheral smear). Nowadays, this process is generally automated by use of an automated analyzer , with only specific samples being examined manually.
Automated blood countComplete blood count performed by an automated analyzer. The blood is well mixed (though not shaken) and placed on a rack in the analyzer. This instrument has many different components to analyze different elements in the blood. The cell counting component counts the numbers and types of different cells within the blood. The results are printed out or sent to a computer for review.
Blood counting machines aspirate a very small amount of the specimen through narrow tubing. Within this tubing, there are sensors that count the number of cells going through it, and can identify the type of cell; this is flow cytometry. The two main sensors used are light detectors, and electrical impedance. One way the instrument can tell what type of blood cell is present is by size. Other instruments measure different characteristics of the cells to categorize them.
Because an automated cell counter samples and counts so many cells, the results are generally very precise. However, certain abnormal cells in the blood may be identified incorrectly, and require manual review of the instrument's results and identify any abnormal cells the instrument could not categorize.
Red cellsTotal red blood cells - The number of red cells is given as an absolute number per microliter (4.2 – 5.6 million per microliter in male and 3.8 – 5.1 in females). Hemoglobin - The amount of hemoglobin in the blood, expressed in grams per deciliter. 14 – 18 grams per deciliter in males and 11 – 16 grams in females) Hematocrit or packed cell volume (PCV) - This is the fraction of whole blood volume that consists of red blood cells (39 – 54 in males and 34 – 47 in females). Note: A microliter occupies the space of a millimeter cubed.
Red blood cell indices Mean corpuscular volume (MCV) - the average volume of the red cells, measured in femtoliters ( 78 – 98 fl) . Anemia is classified as normocytic, microcytic or macrocytic based on whether this value is normal, above or below the expected normal range. (RBC too large – macrocytic too small microcytic )Mean corpuscular hemoglobin (MCH) - the average amount of hemoglobin per red blood cell, in picograms (27 – 35 pg). Mean corpuscular hemoglobin concentration (MCHC) - the average concentration of hemoglobin in the cells (31 – 37%). Red blood cell distribution width (RDW) - a measure of the variation of the RBC population RDW = (Standard deviation of MCV ÷ mean MCV) × 100 Normal 11 – 15%
White Blood CellsATotal white blood cell count is given as the total number of white blood cells per microliter of blood. (normal value varies but generally 4 – 11 thousand per microliter of blood) The CBC also lists the individual types of white blood cells as a percentage or as an absolute number or in cases both. The listing of the individual white blood cell counts is the termed the “differential count.”
Percentages of Leukocytes Figure 17.9
Clinical Terms • Pancytopenia – all blood cells have a low count – generally caused by a aplastic anemia • Erythrocytopenia – too few red blood cells • Erythrocythemia (polycythemia) – too many red blood cells • Leukocytosis – too many total white blood cells • Leukopenia – too few total white blood cells • Thrombocytopenia – too few platelets • Thrombocytosis – too many platelets
Neutropenia – too few neutrophils • Neutrophilia – too many neutrophils • Eosinopenia – too few eosinophils • Eosinophilia – too many eosinophils • Basopenia – too few basophils • Basophilia – too many basophils • Lymphopenia (lymphocytopenia) – too few lymphocytes • Lymphocytosis – too many lymphocytes • Monocytopenia – too few monocytes • Monocytosis – too many monocytes
Erythrocyte/Hemoglobin Disorders • Anemia – blood has abnormally low oxygen-carrying capacity • It is a symptom rather than a disease itself • Blood oxygen levels cannot support normal metabolism • Signs/symptoms include fatigue, paleness, shortness of breath, and chills
Anemia can be due to deficient hemoglobin or hemoglobin that is not functional • Deficient hemoglobin can be caused by inadequate production or increased peripheral destruction • Thus it said that most anemia is due to either decreased production or increased peripheral destruction • The reticulocyte count is used to determine which type it is
Production of New RBC's - Erythropoiesis (takes 4 days) • Hemocytoblasts - Stem cells in the bone marrow from which all blood cells form. • Proerythroblasts - are produced by the division and differentiation of stem cells. 3. Basophilic (early) erythroblasts - During this stage in erythropoiesis hemoglobin synthesis begins. 4. Intermediate erythroblasts - At this time, we see the accumulation of hemoglobin due to its continued synthesis. 5. Late erythroblasts - During this stage the nucleus is extruded from the cell. 6. Reticulocyte - These cells exhibit a net-like appearance or reticulum in their cytoplasm when stained. A small number of reticulocytes (only 1 to 3% of the circulating red cells) are found in the circulation. 7. Mature erythrocytes - At this final stage of maturation there is a loss of ribosomes. These cells enter the circulation.
Examples of increased peripheral destruction are hemorrhage, splenomegaly and others • Examples of decreased production iron deficiency anemia, pernicious anemia, folic acid deficiency • Some decreased production anemias can be microcytic or macrocytic
Non-functional hemoglobin can be as a result of problems with the protein globin as in sickle cell anemia, the thalassemias, and others • Non-functional hemoglobin can also be a result of problems with heme like the iron not being in the +2 oxidation state – but rather in the +3 oxidation state – as a result of being oxidized by a free radical or other chemical entity. O2 can only be carried on the iron of hemoglobin if it is in the +2 oxidation state. All of us have some of our iron in the +3 oxidation state that is it is said a gram of Hgb. Will carry 1.34 ml. of O2 rather that its ideal value of 1.39. If a significant amount of Hgb. In an individual in in the +3 oxidation state such that it lowers the O2 content of the blood below normal – the patient has Methemoglobinemia
Polycythemia • Polycythemia – excess RBCs that increase blood viscosity • Three main polycythemias are: • Polycythemia vera – generally occurs in those over 60 and has no known cause – increase in all the blood cells as a result of an increased action of the pluripotential stem cells – but particularly the RBCs • Secondary polycythemia – due to an increased erythropoietin level secondary to high altitudes, chronic pulmonary disease, CHF, heavy smoking, abnormal hemoglobins that have high O2 affinity • Blood doping • Relative polycythemia
Leukocytosis • Leukocytosis is very common in acutely ill patients. It occurs in response to a wide variety of conditions, including viral, bacterial, fungal, or parasitic infection, cancer, hemorrhage, and exposure to certain medications or chemicals including steroids. Leukocytosis can also be the first indication of neoplastic growth of leukocytes. • For lung diseases such as pneumonia and tuberculosis, WBC count is very important for the diagnosis of the disease, as leukocytosis is usually present. • The mechanism that causes leukocytosis can be of several forms: an increased release of leukocytes from bone marrow storage pools, decreased margination of leukocytes onto vessel walls, decreased extravasation of leukocytes from the vessels into tissues, or an increase in number of precursor cells in the marrow.
Leukopenia • Low white cell counts are associated with chemotherapy, radiation therapy, leukemia (as malignant cells overwhelm the bone marrow), myelofibrosis and aplastic anemia (failure of white and red cell creation, along with poor platelet production). In addition, many common medications can cause leukopenia (eg. minocycline, a commonly prescribed antibiotic). • Other causes of low white blood cell count include: Influenza, systemic lupus erythematosus, Hodgkin's lymphoma, some types of cancer, typhoid, malaria, tuberculosis, dengue, Rickettsial infections, enlargement of the spleen, folate deficiencies, psittacosis and sepsis. Many other causes exist, such as a deficiency in certain minerals such as copper and zinc.
Neutrophilia • Neutrophils are the primary white blood cells that respond to a bacterial infection, so the most common cause of neutrophilia is a bacterial infection. • Neutrophils are also increased in any acute inflammation, so will be raised with appendicitis and after a heart attack or other infarct. • Drugs, such as prednisone, have the same effect as cortisol, causing marginated neutrophils to enter the blood stream. Nervousness will very slightly raise the neutrophil count because of this effect. Exercise also raises the count. • A neutrophilia might also be the result of a malignancy. Chronic myelogenous leukemia (CML or chronic myeloid leukemia) is a disease where the blood cells proliferate out of control.
"Left shift" • A "left shift" refers to the presence of increased proportions of younger, less well differentiated neutrophils and neutrophil-precursor cells in the blood. This generally reflects early or premature release of myeloid cells from the bone marrow, the site where neutrophils are generated. A severe neutrophilia with left shift is referred to as a leukemoid reaction. The leukocyte alkaline phosphatase (LAP) score, which refers to the amount of alkaline phosphatase per neutrophil, will increase. In a severe infection, toxic granulation changes happen to the neutrophils.