Download
1 / 1
10 likes | 232 Vues
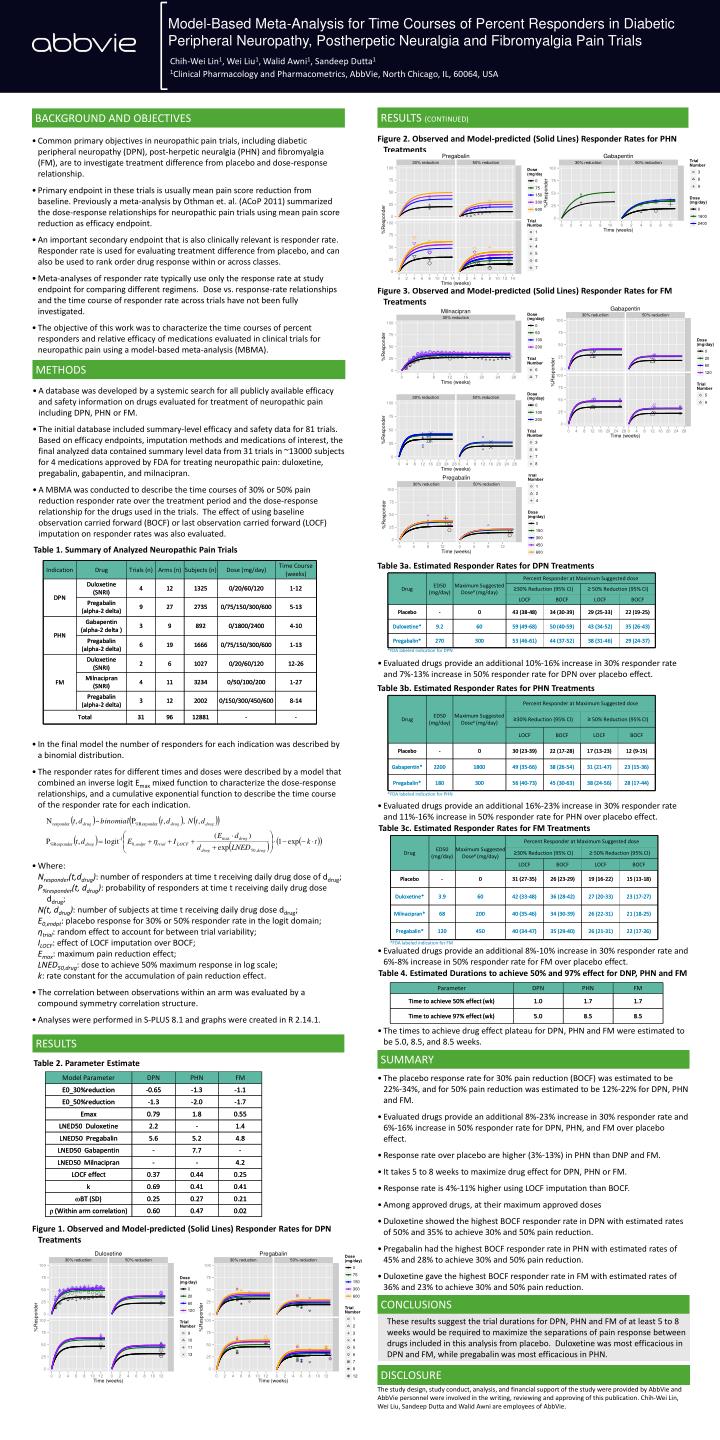
Model-Based Meta-Analysis for Time Courses of Percent Responders in Diabetic Peripheral Neuropathy, Postherpetic Neuralgia and Fibromyalgia Pain Trials. Chih-Wei Lin 1 , Wei Liu 1 , Walid Awni 1 , Sandeep Dutta 1 1 Clinical Pharmacology and Pharmacometrics, AbbVie, North Chicago, IL, 60064, USA.

E N D
Model-Based Meta-Analysis for Time Courses of Percent Responders in Diabetic Peripheral Neuropathy, Postherpetic Neuralgia and Fibromyalgia Pain Trials Chih-Wei Lin1, Wei Liu1, Walid Awni1, Sandeep Dutta1 1Clinical Pharmacology and Pharmacometrics, AbbVie, North Chicago, IL, 60064, USA RESULTS (CONTINUED) BACKGROUND AND OBJECTIVES Figure 2. Observed and Model-predicted (Solid Lines) Responder Rates for PHN Treatments • Common primary objectives in neuropathic pain trials, including diabetic peripheral neuropathy (DPN), post-herpetic neuralgia (PHN) and fibromyalgia (FM), are to investigate treatment difference from placebo and dose-response relationship. • Primary endpoint in these trials is usually mean pain score reduction from baseline. Previously a meta-analysis by Othman et. al. (ACoP 2011) summarized the dose-response relationships for neuropathic pain trials using mean pain score reduction as efficacy endpoint. • An important secondary endpoint that is also clinically relevant is responder rate. Responder rate is used for evaluating treatment difference from placebo, and can also be used to rank order drug response within or across classes. • Meta-analyses of responder rate typically use only the response rate at study endpoint for comparing different regimens. Dose vs. response-rate relationships and the time course of responder rate across trials have not been fully investigated. • The objective of this work was to characterize the time courses of percent responders and relative efficacy of medications evaluated in clinical trials for neuropathic pain using a model-based meta-analysis (MBMA). Figure 3. Observed and Model-predicted (Solid Lines) Responder Rates for FM Treatments METHODS • A database was developed by a systemic search for all publicly available efficacy and safety information on drugs evaluated for treatment of neuropathic pain including DPN, PHN or FM. • The initial database included summary-level efficacy and safety data for 81 trials. Based on efficacy endpoints, imputation methods and medications of interest, the final analyzed data contained summary level data from 31 trials in ~13000 subjects for 4 medications approved by FDA for treating neuropathic pain: duloxetine, pregabalin, gabapentin, and milnacipran. • A MBMA was conducted to describe the time courses of 30% or 50% pain reduction responder rate over the treatment period and the dose-response relationship for the drugs used in the trials. The effect of using baseline observation carried forward (BOCF) or last observation carried forward (LOCF) imputation on responder rates was also evaluated. Table 1. Summary of Analyzed Neuropathic Pain Trials Table 3a. Estimated Responder Rates for DPN Treatments • Evaluated drugs provide an additional 10%-16% increase in 30% responder rate and 7%-13% increase in 50% responder rate for DPN over placebo effect. Table 3b. Estimated Responder Rates for PHN Treatments • In the final model the number of responders for each indication was described by a binomial distribution. • The responder rates for different times and doses were described by a model that combined an inverse logit Emax mixed function to characterize the dose-response relationships, and a cumulative exponential function to describe the time course of the responder rate for each indication. • Evaluated drugs provide an additional 16%-23% increase in 30% responder rate and 11%-16% increase in 50% responder rate for PHN over placebo effect. Table 3c. Estimated Responder Rates for FM Treatments • Where:Nresponder(t,ddrug): number of responders at time t receiving daily drug dose of ddrug;P%responder(t, ddrug): probability of responders at time t receiving daily drug dose ddrug;N(t, ddrug): number of subjects at time t receiving daily drug dose ddrug;E0,endpt: placebo response for 30% or 50% responder rate in the logit domain; ηtrial: random effect to account for between trial variability;ILOCF: effect of LOCF imputation over BOCF; Emax: maximum pain reduction effect;LNED50,drug: dose to achieve 50% maximum response in log scale; k: rate constant for the accumulation of pain reduction effect. • The correlation between observations within an arm was evaluated by a compound symmetry correlation structure. • Analyses were performed in S-PLUS 8.1 and graphs were created in R 2.14.1. • Evaluated drugs provide an additional 8%-10% increase in 30% responder rate and 6%-8% increase in 50% responder rate for FM over placebo effect. Table 4. Estimated Durations to achieve 50% and 97% effect for DNP, PHN and FM • The times to achieve drug effect plateau for DPN, PHN and FM were estimated to be 5.0, 8.5, and 8.5 weeks. RESULTS SUMMARY Table 2. Parameter Estimate • The placebo response rate for 30% pain reduction (BOCF) was estimated to be 22%-34%, and for 50% pain reduction was estimated to be 12%-22% for DPN, PHN and FM. • Evaluated drugs provide an additional 8%-23% increase in 30% responder rate and 6%-16% increase in 50% responder rate for DPN, PHN, and FM over placebo effect. • Response rate over placebo are higher (3%-13%) in PHN than DNP and FM. • It takes 5 to 8 weeks to maximize drug effect for DPN, PHN or FM. • Response rate is 4%-11% higher using LOCF imputation than BOCF. • Among approved drugs, at their maximum approved doses • Duloxetine showed the highest BOCF responder rate in DPN with estimated rates of 50% and 35% to achieve 30% and 50% pain reduction. • Pregabalin had the highest BOCF responder rate in PHN with estimated rates of 45% and 28% to achieve 30% and 50% pain reduction. • Duloxetine gave the highest BOCF responder rate in FM with estimated rates of 36% and 23% to achieve 30% and 50% pain reduction. Figure 1. Observed and Model-predicted (Solid Lines) Responder Rates for DPN Treatments CONCLUSIONS These results suggest the trial durations for DPN, PHN and FM of at least 5 to 8 weeks would be required to maximize the separations of pain response between drugs included in this analysis from placebo. Duloxetine was most efficacious in DPN and FM, while pregabalin was most efficacious in PHN. DISCLOSURE The study design, study conduct, analysis, and financial support of the study were provided by AbbVie and AbbVie personnel were involved in the writing, reviewing and approving of this publication. Chih-Wei Lin, Wei Liu, Sandeep Dutta and Walid Awni are employees of AbbVie.