Download
1 / 1
10 likes | 214 Vues
Measurement of Dose to Critical Structures Surrounding the Prostate from Intensity-Modulated Radiation Therapy (IMRT) and Three Dimensional Conformal Radiation Therapy (3D-CRT); A Comparative Study Erik Frija M.A., Charles E. Poole B.S., R.T. (T), Chris Spicer R.T. (R)(T), C.M.D.

E N D
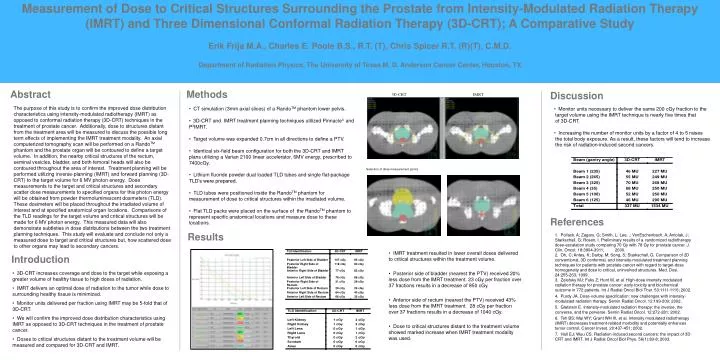
Measurement of Dose to Critical Structures Surrounding the Prostate from Intensity-Modulated Radiation Therapy (IMRT) and Three Dimensional Conformal Radiation Therapy (3D-CRT); A Comparative Study Erik Frija M.A., Charles E. Poole B.S., R.T. (T), Chris Spicer R.T. (R)(T), C.M.D. Department of Radiation Physics, The University of Texas M. D. Anderson Cancer Center, Houston, TX Methods Abstract Discussion The purpose of this study is to confirm the improved dose distribution characteristics using intensity-modulated radiotherapy (IMRT) as opposed to conformal radiation therapy (3D-CRT) techniques in the treatment of prostate cancer. Additionally, dose to structures distant from the treatment area will be measured to discuss the possible long term effects of implementing the IMRT treatment modality. An axial computerized tomography scan will be performed on a RandoTM phantom and the prostate organ will be contoured to define a target volume. In addition, the nearby critical structures of the rectum, seminal vesicles, bladder, and both femoral heads will also be contoured throughout the area of interest. Treatment planning will be performed utilizing inverse-planning (IMRT) and forward planning (3D-CRT) to the target volume for 6 MV photon energy. Dose measurements to the target and critical structures and secondary scatter dose measurements to specified organs for this photon energy will be obtained from powder thermoluminescent dosimeters (TLD). These dosimeters will be placed throughout the irradiated volume of interest and at specified anatomical organ locations. Comparisons of the TLD readings for the target volume and critical structures will be made for 6 MV photon energy. This measured data will also demonstrate subtleties in dose distributions between the two treatment planning techniques. This study will evaluate and conclude not only a measured dose to target and critical structures but, how scattered dose to other organs may lead to secondary cancers. • CT simulation (3mm axial slices) of a RandoTM phantomlower pelvis. • 3D-CRT and IMRT treatment planning techniques utilized Pinnacle3 and P3IMRT. • Target volume was expanded 0.7cm in all directions to define a PTV. • Identical six-field beam configuration for both the 3D-CRT and IMRT plans utilizing a Varian 2100 linear accelerator, 6MV energy, prescribed to 7400cGy. • Lithium fluoride powderdual loadedTLD tubes and single flat-package TLD’s were prepared. • TLD tubes were positioned inside the RandoTM phantom for measurement of dose to critical structures within the irradiated volume. • Flat TLD packs were placed on the surface of the RandoTM phantom to represent specific anatomical locations and measure dose to these locations. • Monitor units necessary to deliver the same 200 cGy fraction to the • target volume using the IMRT technique is nearly five times that • of 3D-CRT. • Increasing the number of monitor units by a factor of 4 to 5 raises • the total body exposure. As a result, these factors will tend to increase • the risk of radiation-induced second cancers. References Results • 1. Pollack, A; Zagars, G; Smith, L; Lee, .; VonEschenbach, A; Antolak, J; Starkschall, G; Rosen, I. Preliminary results of a randomized radiotherapy dose-escalation study comparing 70 Gy with 78 Gy for prostate cancer. J. Clin. Oncol. 18:3904-3911; 2000. • 2. Oh, C; Antes, K; Darby, M; Song, S; Starkschall, G. Comparison of 2D conventional, 3D conformal, and intensity-modulated treatment planning techniques for patients with prostate cancer with regard to target-dose homogeneity and dose to critical, uninvolved structures. Med. Dosi. 24:255-263; 1999. • 3. Zelefsky MJ; Fuks Z; Hunt M, et al. High-dose intensity modulated radiation therapy for prostate cancer: early toxicity and biochemical outcome in 772 patients. Int J Radiat Oncol Biol Ther. 53:1111-1116; 2002. • 4. Purdy JA. Dose-volume specification: new challenges with intensity-modulated radiation therapy. Semin Radiat Oncol. 12:199-209; 2002. • 5. Glatstein E. Intensity-modulated radiation therapy: the inverse, the converse, and the perverse. Semin Radiat Oncol. 12:272-281; 2002. • 6. Teh BS; Mai WY; Grant WH III, et al. Intensity modulated radiotherapy (IMRT) decreases treatment-related morbidity and potentially enhances tumor control. Cancer Invest. 20:437-451; 2002. • 7. Hall EJ; Wuu CS. Radiation-induced second cancers: the impact of 3D-CRT and IMRT. Int J Radiat Oncol Biol Phys. 56(1):83-8; 2003. • IMRT treatment resulted in lower overall doses delivered to critical structures within the treatment volume. • Posterior side of bladder (nearest the PTV) received 20% less dose from the IMRT treatment. 23 cGy per fraction over 37 fractions results in a decrease of 850 cGy. • Anterior side of rectum (nearest the PTV) received 43% less dose from the IMRT treatment. 28 cGy per fraction over 37 fractions results in a decrease of 1040 cGy. • Dose to critical structures distant to the treatment volume showed marked increase when IMRT treatment modality was used. Introduction • 3D-CRT increases coverage and dose to the target while exposing a greater volume of healthy tissue to high doses of radiation. • IMRT delivers an optimal dose of radiation to the tumor while dose to surrounding healthy tissue is minimized. • Monitor units delivered per fraction using IMRT may be 5-fold that of 3D-CRT. • We will confirm the improved dose distribution characteristics using IMRT as opposed to 3D-CRT techniques in the treatment of prostate cancer. • Doses to critical structures distant to the treatment volume will be measured and compared for 3D-CRT and IMRT.



















