Download
1 / 9
90 likes | 95 Vues
Learn about a new approach to research posters that aims to fix the problems with traditional formats. Watch the discussion in NEJM Journal Watch and design your own poster on YouTube.

E N D
A New Creative Option for Research Posters See discussion in NEJM Journal Watch The Problem with Research Posters — and a Bold Approach to Fixing Them Learn more at youtube Click here to design your poster.
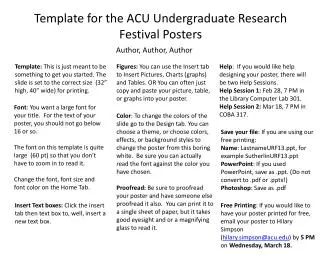
Non-Cognitive Predictors of Student Success:A Predictive Validity Comparison Between Domestic and International Students Non-Cognitive Predictors of Student Success:A Predictive Validity Comparison Between Domestic and International Students Title:Subtitle • AMMO BAR • Delete this and replace it with your… • Extra Graphs • Extra Correlation tables • Extra Figures • Extra nuance that you’re worried about leaving out. • Keep it messy! This section is just for you. Leeroy Jenkins, author2, author3, author4 • INTRO • Just give context for the gap you’re filling • You’re not going to get yelled at if you don’t cite the 5 papers from 1937 that defined this construct. They’ll download your paper if they want that. • METHODS • N = ###, • Collected this • Tested with X statistical test • RESULTS • Graph or table with essential results only. • All the other correlations in the ammo bar. • DISCUSSION • “If this result actually generalized and I didn’t have to humbly disclaim the possibility of a thousand confounds and limitations, it would imply that….” • Keep font size as high above 28 as possible. Main finding goes here, translated into plain English. Emphasize the important words. Take a picture to download thefull paper
Notes • In Powerpoint, click View > Guides • Keep text within gutter guides. • Author list: Don’t split names onto two lines (e.g., “Jimmy [break] Smith”). If that happens, use a new line, unless you need the space. Bold the first names of anybody who’s presenting in person. • Intro/methods/result: Do not drop below font size 28, but if you have extra space, jack up the font size until the space is full. • Do not use color in the sidebars except in graphs/figures. It’ll pull attention from the center and slow interpretation for passersby.
NotesCorrect fonts won’t load until you open this in PowerPoint(e.g., if you’re previewing this in your browser it’ll look uglier than it actually is).
QR FAQ How do I create a QR code? • https://www.qrcode-monkey.com/is free, URLs don’t expire, and you can add cool features like images. How do I scan a QR code? • Just pull out your phone and take a picture!All modern iPhones and most Android phones have built-in QR detection in their cameras. Some Android phones may need an app. How can I link the QR to my paper and a copy of my poster and my contact details. • Try creating a multi-page link for free via https://linktr.ee/. (Still trying to figure out the best answer to this though.) Check out this link to watch a video on scanning #betterposter QR codes. Donated by@kristinrojasmd https://twitter.com/kristinrojasmd/status/1124418213050298368 https://youtu.be/1RwJbhkCA58
Layout FAQ Colors Use these color codes What if my intro/methods/results doesn’t ft in the silent bar? • If you’re trying to put so much into that bar that it doesn’t fit, they won’t have time to read it anyway. First try moving stuff to the ammo bar. Next, cut cutcut. • Instead of trying to fill space, you’re trying to conserve space. What if I have a really important graph or picture? • Move the QR Code to the Silent Presenter, then put your graph/image in the middle.
We Don’t Have to Pick a Side: The Middle Is A Fine Place to Be Andrew R. Smith Community Memorial Health SystemVentura, California Why must we pick sides? The new poster format is a revolution, or the new poster format is garbage!Take the good parts of the new format, keep the useful aspects of the traditional format, add in your own ideas, and create something better. • INTRODUCTION • Mike Morrison created a template for a “Better Scientific Poster” (BSP) (https://osf.io/ef53g/) • The BSP format has been praised by many, yet disparaged by others. • The current project had 2 goals: • Create a template that I think could be useful. • Point out that we don’t need to either love or hate the new format—the middle is just fine. • METHOD • To create a new template, I identified strengths of the BSP template and the traditional format. • BSP strengths: clear take-away message, minimal text, QR code • Traditional format strengths: room for figures, reasonable text size on sides, large title to make finding posters in poster session easy, web link and email for people who don’t like QR codes • RESULTS • Preregistered analysis: 78% increase in liking compared to traditional format and 24% increase compared to the BSP format. • Exploratory analysis: room for improvement in this template (Arial font, seriously?!?!). • DISCUSSION • Sometimes it makes sense to pick a side; this is not one of those times. • Praise what you like, make suggestions for improvement, and then make something better. • Take Mike’s ideas, incorporate some of mine, be creative, and let’s make posters more useful. Poster template: https://osf.io/ayjzg/ smithar3@appstate.edu
Crystalizing ColitisT. Lai, D.O., B. Barrows, D.O., M. Salehpour, M.D., A. Frugoli D.O.COMMUNITY MEMORIAL HEALTH CENTER, VENTURA, CALIFORNIA Ventura, California End-stage renal disease is associated with multiple metabolic and electrolyte derangements. Hormonal and electrolyte imbalance of calcium, phosphorus, and parathyroid hormone (PTH) can result in short term complications,such as calciphylaxis and long term sequelae, such as renal osteodystrophy. As a result, many patients have strict dietary constraints and despite compliance, phosphate binders such as calcium acetate and/or sevelamer carbonate (Renvela) are also needed to treat secondary hyperparathyroidism. This case vignette describes an under recognized adverse effect of a phosphate binder, Renvela induced colitis. Histologic features classically associated with ischemic colitis include marked surface epithelial injury, mucin loss in crypts (atrophic microcrypts), and hyalinization of the lamina propria. The typical lamina propria connective tissue (loose stroma with plasma cells, lymphocytes, and eosinophils) is replaced with a dense eosinophilic matrix and the residual glands become more closely approximated (lamina propria “collapse”). INTRODUCTION FEATURES OF ISCHEMIC COLITIS KAYEXALATE CRYSTALS SEVELAMER CRYSTAL A 47 year old male with insulin dependent diabetes complicated by end-stage renal disease presented with a two day history of abdominal pain with associated nausea. Of note, he presented one month prior with similar symptoms. During his previous admission he underwent evaluation with CT imaging followed by colonoscopy and was found to have numerous circumferential lesions inconsistent with inflammatory bowel disease and attributed to possible ischemia. He was provided supportive care and non-operative management and was discharged home. He returned with similar symptoms one month later. He was empirically started on antimicrobials and underwent additional evaluation with repeat imaging using CT mesenteric angiogram, which demonstrated colitis in the distal ascending, transverse and proximal descending colon with pericolic stranding but no evidence of atherosclerotic disease. He underwent repeat colonoscopy that re-identified 3 areas of circumferential ulceration in the ascending/hepatic flexure, splenic flexure and descending colon. Pathology report noted necrotic tissue and ulcerative debris with non-polarizing crystalline material from biopsies taken from the areas of ulceration. Evaluation for additional causes, including cardioembolic events and vasculitis, were bland. Review of prior pathology and current biopsy specimens demonstrated crystalline material most likely related to Renvela use. Renvela was discontinued, and the patient was transitioned to calcium carbonate. His symptoms improved with cessation of Renvela and initiation of the calcium-based phosphate binder. This vignette describes a rare adverse effect of sevelamer carbonate therapy. Review of the literature shows a limited number of reported cases. Additionally, cases of Renvela resin related necrosis can be misidentified with cases of Kayxelate or bile acid sequestrants, as all represent medication resin resulting in colonic necrosis. Pathologists are able to distinguish Kayexalate’s morphology from Renvela as it is rectangular with internal demarcation described as “fish scales,” with a very characteristic hue that was described by Gonzales et al & Swanson et al, 2017. Given the very small incidence, no definitive pathophysiology has been confirmed and only limited reports of pathologic identification exists. We offer review of the pathologic tissue finding, as well as a proposed mechanism oftissue injury. Both kayexalate and sevelamer crystals show similar histomorphology with characteristic “fish scale” pattern on H&E stained slides. Both crystals are also non-polarizable under polarized light microscopy. The only differentiating characteristics between the two crystals is the pigmentation after standard H&E staining. Kayexalate shows basophilic pigmentation, and sevelamer demonstrates characteristic yellow/gold coloration. SEVELAMER VS. KAYEXALATE CRYSTAL MORPHOLOGY CASE PRESENTATION DISCUSSION Both sevelamer and kayexalate associated colitis show histologic features which can mimic ischemic colitis. These features include marked surface epithelial injury, mucin loss in crypts (atrophic microcrypts), and hyalinization of the lamina propria. The typical lamina propria connective tissue (loose stroma with plasma cells, lymphocytes, and eosinophils) is replaced with a dense eosinophilic matrix and the residual glands become more closely approximated (lamina propria “collapse”). This highlights the importance of clinical history and identification of crystals on H&E stains to prevent the incorrect diagnosis of ischemic colitis in the setting of what could potentially be a drug associated reaction. Both sevelamer and kayexalate associated gastrointestinal injury generally resolve with cessation of medication. SEVELAMER AND KAYEXALATE ASSOCIATED COLITIS SEVELAMER ASSOCIATED COLITIS 1. R. Gonzalez, MD, S. Lagana, MD, O. Szeto, MD et al. Challenges in Diagnosing Medication Resins in Surgical Pathology Specimens. Arch Pathol Lab Med—Vol 141, September 2017. 2. C. Yuste1, E. Me´rida, E. Hernandez et al. Gastrointestinal complications induced by sevelamer crystals. Clinical Kidney Journal, 2017, vol. 10, no. 4, 539–544. 3. C. E. McGowan, MD, S. Saha, MD, G. Chu, MD et al. Intestinal Necrosis due to Sodium Polystyrene Sulfonate(Kayexalate) in Sorbitol. South Med J. 2009 May ; 102(5): 493–497. 4. B. Swanson, B. Limketkai ,T. Liu et al. Sevelamer crystals in the Gastrointestinal Tract (GIT) a new entity associated with mucosal injury. Am J Surg Pathol 2013; 37: 1686–169. REFERENCES SEVELAMER ASSOCIATED COLITIS WITH FEATURES MIMICKING ISCHEMIC COLITIS