Download
1 / 1
10 likes | 132 Vues
Dual Antiplatelet Agent Failure: A New Syndrome or a Clinical Non-Entity? Geoffrey D. Barnes, Jin Li, Eva Kline-Rogers, Rebecca Juliar, David F. Armstrong, James B. Froehlich, MD, Kim A. Eagle, MD, Hitinder S. Gurm , MD, University of Michigan Medical Center, Ann Arbor, MI. METHODS. ABSTRACT.

E N D
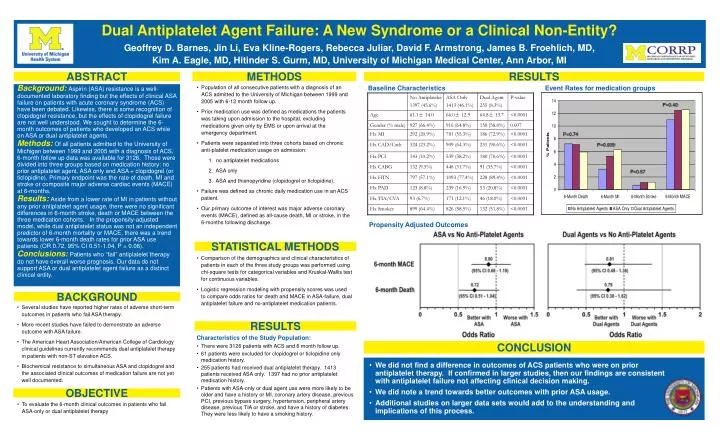
Dual Antiplatelet Agent Failure: A New Syndrome or a Clinical Non-Entity? Geoffrey D. Barnes, Jin Li, Eva Kline-Rogers, Rebecca Juliar, David F. Armstrong, James B. Froehlich, MD, Kim A. Eagle, MD, Hitinder S. Gurm, MD, University of Michigan Medical Center, Ann Arbor, MI METHODS ABSTRACT RESULTS Background:Aspirin (ASA) resistance is a well-documented laboratory finding but the effects of clinical ASA failure on patients with acute coronary syndrome (ACS) have been debated. Likewise, there is some recognition of clopidogrel resistance, but the effects of clopidogrel failure are not well understood. We sought to determine the 6-month outcomes of patients who developed an ACS while on ASA or dual antiplatelet agents. Methods:Of all patients admitted to the University of Michigan between 1999 and 2005 with a diagnosis of ACS, 6-month follow up data was available for 3126. Those were divided into three groups based on medication history: no prior antiplatelet agent, ASA only and ASA + clopidogrel (or ticlopidine). Primary endpoint was the rate of death, MI and stroke or composite major adverse cardiac events (MACE) at 6-months. Results:Aside from a lower rate of MI in patients without any prior antiplatelet agent usage, there were no significant differences in 6-month stroke, death or MACE between the three medication cohorts. In the propensity-adjusted model, while dual antiplatelet status was not an independent predictor of 6-month mortality or MACE, there was a trend towards lower 6-month death rates for prior ASA use patients (OR 0.72, 95% CI 0.51-1.04, P = 0.08). Conclusions:Patients who “fail” antiplatelet therapy do not have overall worse prognosis. Our data do not support ASA or dual antiplatelet agent failure as a distinct clinical entity. • Population of all consecutive patients with a diagnosis of an ACS admitted to the University of Michigan between 1999 and 2005 with 6-12 month follow up. • Prior medication use was defined as medications the patients was taking upon admission to the hospital, excluding medications given only by EMS or upon arrival at the emergency department. • Patients were separated into three cohorts based on chronic anti-platelet medication usage on admission: 1. no antiplatelet medications 2. ASA only 3. ASA and thienopyridine (clopidogrel or ticlopidine). • Failure was defined as chronic daily medication use in an ACS patient. • Our primary outcome of interest was major adverse coronary events (MACE), defined as all-cause death, MI or stroke, in the 6-months following discharge. Baseline Characteristics Event Rates for medication groups P=0.40 P=0.74 P=0.009 P=0.57 Propensity Adjusted Outcomes STATISTICAL METHODS • Comparison of the demographics and clinical characteristics of patients in each of the three study groups was performed using chi-square tests for categorical variables and Kruskal-Wallis test for continuous variables. • Logistic regression modeling with propensity scores was used to compare odds ratios for death and MACE in ASA-failure, dual antiplatelet failure and no-antiplatelet medication patients. BACKGROUND • Several studies have reported higher rates of adverse short-term outcomes in patients who fail ASA therapy. • More recent studies have failed to demonstrate an adverse outcome with ASA failure. • The American Heart Association/American College of Cardiology clinical guidelines currently recommends dual antiplatelet therapy in patients with non-ST elevation ACS. • Biochemical resistance to simultaneous ASA and clopidogrel and the associated clinical outcomes of medication failure are not yet well documented. RESULTS • Characteristics of the Study Population: • There were 3126 patients with ACS and 6 month follow up. • 61 patients were excluded for clopidogrel or ticlopidine only medication history. • 255 patients had received dual antiplatelet therapy. 1413 patients received ASA only. 1397 had no prior antiplatelet medication history. • Patients with ASA-only or dual agent use were more likely to be older and have a history or MI, coronary artery disease, previous PCI, previous bypass surgery, hypertension, peripheral artery disease, previous TIA or stroke, and have a history of diabetes. They were less likely to have a smoking history. CONCLUSION • We did not find a difference in outcomes of ACS patients who were on prior antiplatelet therapy. If confirmed in larger studies, then our findings are consistent with antiplatelet failure not affecting clinical decision making. • We did note a trend towards better outcomes with prior ASA usage. • Additional studies on larger data sets would add to the understanding and implications of this process. OBJECTIVE • To evaluate the 6-month clinical outcomes in patients who fail ASA-only or dual antiplatelet therapy



















