Download
1 / 27
270 likes | 330 Vues
Rheumatic Fever. Dr.Emamzadegan Pediatric Cardiologist. Rheumatic Fever. 1 . Etiology : As many as 2/3 of the patients with an acute episode of rheumatic fever have a history of an upper respiratory tract infection (GAS) several weeks before. Etiology.

E N D
Rheumatic Fever Dr.Emamzadegan Pediatric Cardiologist
Rheumatic Fever 1.Etiology: As many as 2/3 of the patients with an acute episode of rheumatic fever have a history of an upper respiratory tract infection (GAS) several weeks before.
Etiology “”Patients with acute rheumatic fever almost always have serologic evidence of a recent GAS infection. “”Their antibody titers are usually considerably higher than those seen in patients with GAS infections without acute rheumatic fever.
Etiology “”Not all of the serotypes of GAS can cause rheumatic fever. “”Certain serotypes of GAS (M types 1, 3, 5, 6, 18,24) are more frequently isolated from patients with acute rheumatic fever than are other serotypes. M4 = no RF
Epidemiology “”Worldwide, rheumatic heart disease remains the most common form of acquired heart disease in all age groups. “”The decline in incidence of acute rheumatic fever in industrialized countries over the past 4 decades has also been attributable in large measure to the greater availability of medical care and to the widespread use of antibiotics.
Epidemiology “”Antibiotic therapy of GAS pharyngitis has been important in preventing initial attacks and, particularly, recurrences of the disease. “”In addition, the decline can be attributed, at least in part, to a shift in the prevalent strains of GAS from rheumatogenic to nonrheumatogenic strains.
Epidemiology “”The incidence of both initial attacks and recurrences of acute rheumatic fever peaks in children 5-15 yr of age, the age of greatest risk for GAS pharyngitis. “”In addition, there appears to be a genetic predisposition to acute rheumatic fever.
PATHOGENESIS 1.Cytotoxicitytheory: GAS produces several enzymes that are cytotoxic for mammalian cardiac cells, such as streptolysin 0.
PATHOGENESIS 2.Immunologictheory : Common antigenic determinants are shared between certain components of GAS (M protein, protoplast membrane, cell wall group A carbohydrate, capsular hyaluronate) and specific mammalian tissues (e.g., heart, brain, joint).
Immunologictheory For example, certain M proteins (MI, M5, M6, and M19) share epitopes with human tropomyosin and myosin.
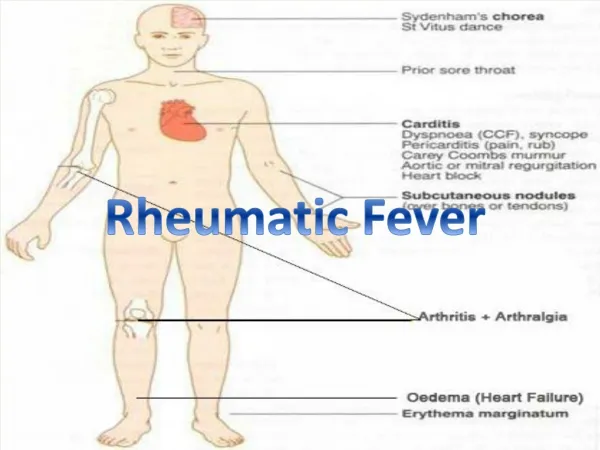
CLINICAL MANIFESTATIONS Jones criteria: A. Major criteria: 1.Migratorypolyarthritis 2.Carditis 3. Sydenham chorea 4. Erythema marginatum 5. Subcutaneous nodules
Jones criteria B. Minor criteria: 1.Fever 2.Arthralgia 3.Elevated ESR,CRP 4.Prolonged PR interval(> 0.2 sec) 5. History of RF
Diagnosis The diagnosis of acute rheumatic fever can be established by the Jones criteria when a patient fulfills 2 major criteria or 1 major and 2 minor criteria.
CLINICAL MANIFESTATIONS 1.Arthritis Migratory; inverse relationship with carditis; larger joints particularly the knees, ankles, wrists, and elbows; hot, red,swollen, and exquisitely tender; dramatic response to even small doses of salicylates;not deforming; Synovial fluid with NL glucose,
CLINICAL MANIFESTATIONS 2.Carditis All of the associated morbidity and mortality; pancarditis; Endocarditis (valvulitis), which manifests by 1 or more cardiac murmurs, is a universal finding in rheumatic carditis; Most cases consist of either isolated mitral valvular disease or combined aortic and mitral valvular disease;
2.Carditis Carditis (tachycardia, cardiomegaly,Murmur, CHF); the major consequence of acute rheumatic carditis is chronic, progressive valvular disease, particularly valvular stenosis, which can require valve replacement and predispose to infective endocarditis. p:1142
Recent Group AStreptococcus Infection “”Acute rheumatic fever typically develops 2-4 wk after an acute episode of GAS pharyngitis. One third of patients have no history of an antecedent pharyngitis. Lab test: If only a single antibody is measured (usually antistreptolysin 0 ) , only 80-85% of patients with acute rheumatic fever have an elevated titer; however,95-100% have an elevation if 3 different antibodies (antistreptolysin 0. anti-DNase B. antihyaluronidase) are measured.
Treatment All patients with acute rheumatic fever should be placed on bed rest and monitored closely for evidence of carditis. They can be allowed to ambulate as soon as the signs of acute inflammation have subsided. However, patients with carditis require longer periods of bed rest.
Treatment 1.Antibiotictherapy: regardless of the throat culture results, the patient should receive 10 days of orally administered penicillin or erythromycin, or a single intramuscular injection of benzathine penicillin to eradicate GAS from the upper respiratory tract. After this initial course of antibiotic therapy, the patient should be started on long-term antibiotic prophylaxis.
Treatment 2. Anti-inflammatory therapy: Patients with typical migratory polyarthritis and those with carditis without cardiomegaly or congestive heart failure should be treated with oral salicylates. The usual dose of aspirin is 100 mg/kg/day in 4 divided doses PO for 3-5 days, followed by 75 mg/kg/day in 4 divided doses PO for 4 wk.
2. Anti-inflammatory therapy: Patients with carditis and cardiomegaly or congestive heart failure should receive corticosteroids. With moderate to severe carditis: Diuretics,fluid & salt restriction,digoxin,o2
Treatment Sydenham Chorea: Anti-inflammatory agents are usually not indicated, phenobarbital (16-32 mg every 6-8 hr PO) is the drug of choice.(haloperidol, chlorpromazine).
COMPLICATIONS the longterm sequelae of rheumatic fever are usually limited to the heart. The antibiotic regimens used to prevent recurrences of acute rheumatic fever are inadequate for protection against infective endocarditis. Patients who have had rheumatic fever but have no evidence of residual valvular disease do not require endocarditis prophylaxis.
PROGNOSIS It depends on the clinical manifestations present at the time of the initial episode, the severity of the initial episode, and the presence of recurrences. Patients without carditis during the initial episode are unlikely to have carditis with recurrences.
PROGNOSIS patients with chorea, even in the absence of other manifestations of rheumatic fever, require long-term antibiotic prophylaxis.
Prevention 1.Primary prevention: Appropriate antibiotic therapy instituted before the9th day of symptoms of acute GAS pharyngitis is highly effective. However, about 1/3 of patients with acute rheumatic fever do not recall a preceding episode of pharyngitis.
Prevention 2.Secondary Prevention: P:1144