Download
1 / 27
290 likes | 387 Vues
ACUTE RHEUMATIC FEVER. Definition Current Diagnosis 07. An acute systemic immune disease that may develop after an infection with Group A beta- hemolytic Streptococcal infection of the pharynx.

E N D
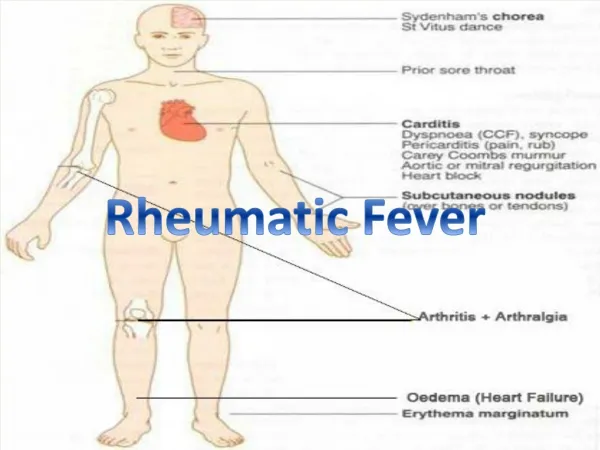
Definition Current Diagnosis 07 • An acute systemic immune disease that may develop after an infection with Group A beta- hemolytic Streptococcal infection of the pharynx. • This disease can affect the HEART, JOINTS, SKIN, SUBCUTANEOUS TISSUE, BRAIN, RESPIRATORY SYSTEM, VESSELS, SEROSAL MEMBRANES, TENDONS AND FASCIAL SHEATHS
GENERAL CONSIDERATIONS • Usually preceded – 2-3 weeks (1-5 weeks) by sore throat. • Peak incidence 5- 15 years. Rare in <4 year olds and > 40 years 3% of pt dev ARF
PATHOLOGY The Aschoff bodies comprises a localised area of inflammation having a central deposit of amorphous fibrinoid material surrounded by an inflammatory infiltrate of mesenchymal cells known as Anitschkow giant cells or “caterpillar cells” (because the chromatin is distributed in the centre of the nucleus in the forrm of a slender wavy ribbon that resemles the attenuated body with innumerable fine leg like projections ) and an occasional multinucleated Aschoff giant cell with”owl eyed” nucleoli Fully developed Aschoff bodies are pathognomonic of RF Aschoff bodies proceed thru 3 phases- exudative, proliferative and healed
MODIFIED JONES’ CRITERIA MAJOR: • Polyarthritis • Carditis • Chorea • Subcutaneous nodules • Erythema marginatum
MINOR CRITERIA Clinical • Fever • Polyarthralgia • h/o previous ARF or Rheum. heart disease Lab • Reversible prolongation of PR interval • Inc ESR • Inc C Reactive Protein • + throat culture Or rapid streptococcal antigen test • Inc ASO titre
POLYARTHRITIS • Migratory – flitting and fleeting • Involves large joints sequentially • Polyarthritis- in adults only a single joint may be affected • Lasts 1-5 weeks • Occurs in 75% or patients • Subsides without residual deformity • Dramatic response of arthritis to therapeutic doses of aspirin or NSAIDs
CARDITIS • Most likely in children and adolescents • Occurs in 1/3 of cases • Any of the following signs suggest the presence of carditis • Endocardial- - MR or AR murmurs indicative of dilatation of valve ring with or without associated valvulitis -Short mid-diastolic murmur (Carey-Coombs) may be present - Changing quality of heart sounds 2. Myocardial - Tachycardia even at rest. Arrhythmias or ectopic beats - Cardiomegaly- on physical exam, CXR or ECHO - Congestive cardiac failure – right or left sided 3. Pericardial - Pericarditis - Pericardial effusion ECG Changes - Changing contour of P waves - Inversion of T waves - Prolongation of PR interval Maybe self limiting or may lead to slowly progressive valvular deformity Mitral valve attacked in 75% cases, aortic in 30% ( but rarely as the sole valve), tricuspid and pulmonary in < 5% cases
SYDENHAM’S CHOREA • Involuntary choreo- athetoid movements primarily of the face, tongue, and upper extremities • Maybe sole manifestation- in 50% of cases no other signs of RF • Girls more frequenty affected • Rare in adults • Lease common(<3%) but most diagnostic of the manifestations of RF
Erythema Marginatum • Rapidly enlarging macules that assume the shape of rings or crescents with clear centres • They may be raised, confluent and either transient or persistent.
Subcutaneous Nodule • Uncommon except in children • Small (<2cm in diameter) firm & nontender • Attached to fascia, or tendon sheaths over bony prominences • Persist for days or weeks • Are recurrent • Indistinguishable from rheumatoid nodules
“Also there” features: • Pneumonia • Epistaxis • Erythema nodosum • Abdominal pain
REQUIRED FOR DIAGNOSIS • Two major criteria OR • One major and two minor criteria
DIFFERENTIAL DIAGNOSIS • Rheumatoid arthritis • Osteomyelitis • Endocarditis • Chronic meningiococcemia • SLE • Lyme disease • Sickle cell disease • Surgical abdomen
TREATMENT PHARYNGITIS Benzathene penicillin 1.2 million units ( 50,000 units/kg to a max of 1.2 million units) is injected IM once or Inj Procaine penicillin 600,000 units once daily for 10 days Erythromycin can be substituted ( 40mg/kg/day) CARDITIS • Bed rest – until temp, ESR, resting pulse rate and ECG have all returned to normal • Prednisone if there is CCF or cardiomegaly POLYARTHRITIS • Anti inflammatory agent - Aspirin markedly reduces fever, joint pain and swelling • No effect on the natural course of the disease • 100mg / kg/day in 4-6 divided doses. Can be reduced to 75mg/Kg/day once there is a response . Given for 4-6 weeks • Toxicity includes- tinnitus, vomiting and GI bleeding. • When response to aspirin is inadequate a short course of prednisone (1 mg/kg/day) orally daily usually causes rapid improvement of joint symptoms. It is tapered over 2 weeks. Add aspirin when tapering begins.
PREVENON OF ARF-PRIMARY • Early and adequate treatment of Strep. throat infections with a penicillin or Azithromycin will prevent Rheumatic Fever • Avoidance of overcrowding & improved hygiene will decrease the incidence of pharyngitis
PREVENTION -SECONDARY Those who have had RF can have recurrences Recurrences are most common in children and in those patients who have had carditis during their initial episode of RF Recurrences are prevented by giving Benzathine penicillin 1.2million units IM every 4 week OR Oral penicillin 250 mg bid Erythromycin 250 mg bid Azithromycin Duration controversial: 5 years after last attack or at 25 years, whichever is later (earlier recommendation: life-long) Those with cardiac involvement and in high risk group- military personnel, health staff, school teachers, parents of young children- life long prophylaxis
RHEUMATIC HEART DISEASE • Results from single or repeated attacks of RF • Rigidity and deformity of valves resulting in stenosis or incompetence or both • Mitral valve alone in 50% • Mitral + Aortic in 25% • Pure aortic uncommon • History of RF obtained in 60% • Should receive prophylatic penicillin monthlyand preceding dental extractions,urologic and surgical procedures to prevent endocarditis