Download
1 / 14
140 likes | 252 Vues
Measuring and scoring cardiac autonomic neuropathy : a first comparison in diabetes. M. Fevre-Genoulaz M.J. Lafitte S.S. Srikanta. Aim of the study.

E N D
Measuring and scoring cardiac autonomic neuropathy : a first comparison in diabetes M. Fevre-Genoulaz M.J. Lafitte S.S. Srikanta
Aim of the study Compare the classification of cardiac autonomic neuropathy (CAN) given by standard autonomic scoring and by a new device : the ANSiscopeTM (Dyansys) in healthy volunteers and in diabetic patients
Study population • 21 type 2 diabetic patients (mean age=50+/-9 yrs). 4 of them had complications due to diabetes : retinopathy, and hypertension • 9 non-diabetic volunteers (mean age 38 +/-9 yrs)
Exclusion criteria • Causes of autonomic neuropathy other than diabetes • History of psychoactive drug or alcohol abuse • Cardiac arrythmia
Methods • Each patient underwent 2 sets of tests : • Autonomic tests • ANSiscopeTM autonomic dysfunction test
Autonomic tests • RSA : respiratory sinus arrythmia • Ratio RR inspiration/RR expiration • Valsalva manoeuver • Ratio longest RR/shortest RR • Systolic blood pressure response to standing • Difference between SBP before and 2 min after standing. • 30:15 ratio • Ratio 30th RR int./15th RR int.
Autonomic tests scoring • Scoring is made following description of Bellavere et al. For each test results are classified as being : • Normal = 0 • Borderline = 1 • Abnormal = 2 • The points are added and final score is interpreted as : • 0 and 1 = healthy • Between 2 and 4 = early CAN • 5 and upper = advanced CAN
Assessment of autonomic scoring • minimum 30 minutes of testing • 45 minutes of signal analysis • Complete patient participation • Trained medical team
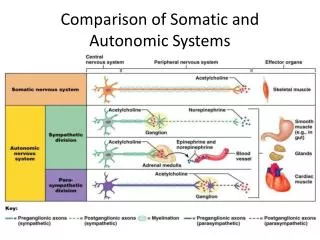
Measurement with the ANSiscopeTM • This device extracts from the RR intervals (recorded with 3 leads ECG) the activity of the sympathetic and parasympathetic systems on a beat by beat basis. • Measurement of dysautonomia is expressed as a lack of coupling between both activites. Result is expressed as a percentage and a group classification.
Measurement conditions with the ANSiscopeTM • A recording of 572 RR intervals is needed (around 5-7 minutes) • Patient must be at rest in supine condition without external stimulation (which may activate sympathetic system).
Classification group • The nature of the groups : aggregation of values • Values demarcating groups • -11.5 to 11.5 : healthy group • 13.5 to 20 : early group • 23 to 50.99 : late group • 51 to 100 : advanced group healthy early late advanced
Results • Number of patients / groups (H = healthy, E = Early, L = late, A = Advanced), (mean average of dysautonomia percentage +/- Std) • Autonomic scoring detected 2 groups of patients : healthy and early CAN • ANSiscopeTM detected 4 stages of CAN in the same set of patients from healthy to most advanced CAN. • If we consider in the ANSiscopeTM classification 2 groups of patients : (healthy + early) and (late + advanced), we obtain :
Results • Non diabetic and diabetic populations have the same proportion of H and E with autonomic scoring • All patients classified with L and A CAN with the ANSiscope have a mean diabetes duration of 7 yrs which predisposes them to CAN. • All diabetics patients with complications are in L + A group. • Some patients without clinical symptoms are in L+A group, these patients may be considered as being at risk to develop complications due to diabetes.
Conclusion • These first results suggest that the ANSiscopeTM allows to detect precociously CAN and classify patients accurately compared to autonomic scoring. • Method is simple, quick and does not require particular training, it thus represents a good tool to measure autonomic neuropathy in clinical practice. • Further studies need to be performed on larger population.