Download
1 / 25
260 likes | 352 Vues
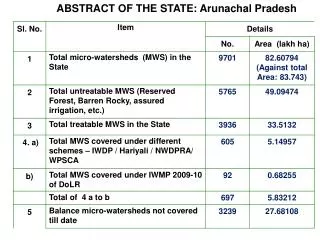
Arunachal Pradesh. 10 th CRM: Arunachal Pradesh. Best Practices: Herbal Garden Initiative @ PHC in Pasighat. Positives. Overall Neat and clean infrastructure. Facilities have boundary walls, at places beautiful bamboo fencing and herbal garden

E N D
Positives • Overall Neat and clean infrastructure. Facilities have boundary walls, at places beautiful bamboo fencing and herbal garden • Dialysis unit: Machine, trained HR and Infrastructure available. • Basic ANC services provided. Early initiation of breast feeding practiced. • C-section available at General Hospital, East Siang and FRU, Ruksin. • Well functioning SNCU • State insurance with coverage up to Rs 2 lakhs for all patients.
Positives contd……. • ASHA : minimal attrition . Almost all ASHAs have bank account. • ANM and GNM school at GH and plans for starting BSc Nursing. • State Quality Assurance structures in place. • Funds being transferred online. HPDs given funds as per norms • Widespread Dengue outbreak in 2015 controlled well: one mortality. • Both the districts have dedicated TB hospitals
Major Findings • HR systems non existent: • Highly irrational posting especially in Sub centres • Ad-hoc recruitment, no skill assessment • Urban Health Centers – a place to accommodate personnel in HQ • Weak supportive supervision • Sub optimal service utilization: assured services not provided in facility and community despite adequate staffing.
Major Findings • Actual requirements of field not reflected in the plans and implementation: • No Micro-plans for VHND and due list for immunization • RNTCP Microscopy centers are under-utilized and cases sent directly to DH • Sub optimal utilization of NCD clinics at DH and CHC • Non Functioning MMU • No Condoms, OCPs, ECPs, Nischay kit in facilities except DH
Major Findings • High Out of pocket expenditure due to non availability of free drugs, diagnostics, dialysis initiatives and weak referral transport system • Districts unclear about Quality Assurance Program, still following ISO • Grievance redressal mechanism not found in any facility • Labour room protocols, partographs not practiced. Labour room nurses rotated every week • ASHA recruited last year, have not got any orientation training. Overall weak training system
Highly irrational posting especially in Sub centres Timeline March 2018 • Transfer order issued vide order No MEST-2016/88 dated Nlg the 13th May 2017 where 118 staffs transferred.(36 ANMs) link • East Siang -one facility namely SCTakilalung where 5 ANM were posted during the visit of 10th CRM team. Now 3 ANMs were posted out on 21st Nov’2016 vide order no. M-5271/T/P/11-12. • HRMIS is being implemented.
Ad-hoc recruitment, no skill assessment Timeline December 2017 • Contractual recruitment done at State HQ & regular through Public Service Commission, • They undergo induction training at State • Undergo continuing training on MH, CH, FP and other program to enhance their skill. • Currently, contractual recruitment on hold. • All recruitment through Public Service Commission only for Doctors. • Other category recruitment through state department central recruitment board (Written, practical & viva) • Recurrent baseline assessment ongoing for Nurses & LT and will scale up to include Doctors also
Urban Health Centers – a place to accommodate personnel in HQ • Current status of staff at UPHC following CRM:- At Pasighat 1 MO, 1 pharma, 2 GNM, 4 ANM, 1 LT, 2 FA, 1 Male Attendant, 1 N/Chowkidar, 1 Sweeper. At Naharlagun/Itanagar Transfer order issued vide order No MEST-2016/88 dated Nlg the 13th May 2017 (118 manpower transferred) Timeline December 2017
Weak supportive supervision • Difficult topography and poor road connectivity impedes on planned supportive supervision. • No proper monitoring vehicle in majority districts. Private vehicles used for Monitoring and supervision. • Supportive supervision plan in place at state • To place S/S plan at district • Technical support from DPs for NHPDs also Timeline December 2017
Sub optimal service utilization: assured services not provided in facility and community despite adequate staffing. • Functionality an issue due to irrational manpower placement • Basics services are provided in all functional SCs. • Beneficiaries prefer going to PHC/CHC/DH. • Functionalisation being initiated through rational posting • Regular review at district level planned • Regular S/S visit is being ensured from district & state • More training on all services ongoing and planned. Timeline September 2017
No Micro-plans for VHND and due list for immunization • Micro-plan for RI in place (Post MI) • 7 districts plan being corrected & improved. • Micro-plan and due list in place during MI rounds • Districts directed to generate due list for RI sessions also • Micro Plan for VHND available in 12 districts & rest furnishing shortly. Timeline September 2017
RNTCP Microscopy centers are under-utilized and cases sent directly to DH • Low population leading to low cases • Cases needing FNAC or complicated looking are referred to DH Timeline August 2017
Sub optimal utilization of NCD clinics at DH and CHC • It is a new programme • Systems to be placed and consolidated in all districts and functionalise clinics in health facilities. • Training ongoing at ToT level Timeline September 2017
Non Functioning MMU • 2 unit MMUs in 16 districts • MMU camp is conducted 6 camps per month (Ave). • MMU specific manpower not in place • Team constituted from among manpower in health facilities • Notice for combining School health mobile teams • Districts with fully non-functional MMUs identified and issued notice. Timeline August 2017
No Condoms, OCPs, ECPs, Nischay kit in facilities except DH • The observation has been reviewed for all districts • FP commodities now in place at districts • Condoms, OCPs, ECPs, Nischay kit received on 28/12/2016 and issued to all the facilities and ASHAs. • Supply chain management need revamping through use of IT (DVDMS) • More training being planned on FP services. Timeline August 2017
High Out of pocket expenditure due to non availability of free drugs, diagnostics, dialysis initiatives and weak referral transport system • The state Govt provides free drugs in the health facilities • State Govt provides fund for procurement of drugs (Health Deptt & DC) • Plan for Free diagnostic services under NHM will be shared during NPCC • PM Dialysis program underway. Tender floated on 30th May 2017 and by August, it should be functional in atleast 3 GHs. • JSSK in operation but need dramatic improvement at facilities • Plan for orientation of MO incharges of all facilities. • Quarterly Review Meeting of districts on NHM Performance at State Chaired by Commissioner (Health & Family Welfare) • Awareness on JSSK, JSY and free referral transport through IEC media including 102 ERC (in Place at Naharlagun) Timeline Dec 2017
Districts unclear about Quality Assurance Program, still following ISO • GH Pasighat was ISO certified. • Quality Assurance cell being improved • More orientation on importance of quality assurance for health staff planned. • Training on Quality assurance to Mos being planned. • Training of assessors, peer planned • Overall, National quality certification of DH planned. Timeline December 2017
Grievance redressal mechanism not found in any facility • Grievanceredressal mechanism through online system 104 EoI already floated. • 104 toll free no for comprehensive grievance (Health information, ASHA and any grievance) • Redressal mechanism is being inbuilt in the call centre. • Effective GR cell will be functionalised on hospitals and then to health facilities Timeline September 2017
Labour room protocols, partographs not practiced. LR nurses rotated every week • Due to shortage of Nurses, roration is practiced. • LR protocols are in place • It is a challenge to ensure use of Partograph even in the hospitals • More Doctors / Nurses are trained in SBA / BeMOC which will improve use. • Several notice issued for permanent posting of nurses to Labour / SNCU / ANC clinic and after 10th CRM too. Timeline Sept 2017
ASHA recruited last year, have not got any orientation training. Overall weak training system • Induction training of newly recruited Rural ASHA and Urban ASHA has been completed. • Orientation training of all existing ASHA done. • ASHA trainings started from Jan’2017. Timeline August 2017