Download
1 / 36
370 likes | 513 Vues
Choices. empower service users and carers with informed choices about options for reducing distress and improving quality of life “the literature makes it abundantly clear that service users want to be offered more than just medication” (Warner, Mariathasan, Lawton-Smith, & Samele, 2006)

E N D
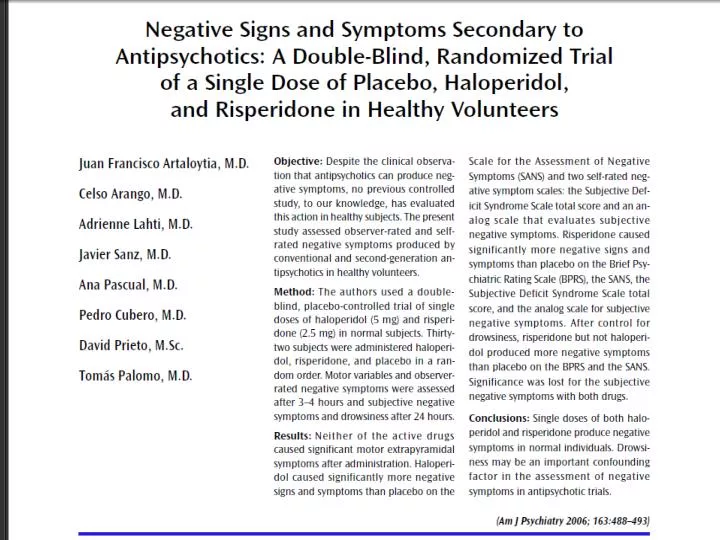
Choices empower service users and carers with informed choices about options for reducing distress and improving quality of life “the literature makes it abundantly clear that service users want to be offered more than just medication” (Warner, Mariathasan, Lawton-Smith, & Samele, 2006) Choosing not to take antipsychotics may be a rational decision in relation to cost-benefit profile
Our Approach • To increase awareness in primary care services, secondary care services, voluntary sector, further education and the community • Increase referrals through • Training for potential referrers • Rapid response • Flexible approach to clients • Positive, user friendly service • Use of cognitive therapy
Can a cognitive model be applied to distressing psychotic experiences?
On the next slide carry out the following instructions • Stare at the blue dots while you count slowly to 30. • Then close your eyes and tilt your head back. A circle of light will slowly appear. Keep looking at it. • What do you see?
What is schizophrenia? two or more of: delusions, hallucinations, disorganised speech, grossly disorganised/catatonic behaviour, negative symptoms (flat affect, poverty of speech, avolition) social/occupational dysfunction - at least one of work/interpersonal relationships/self-care at least 6 months (with at least 1 month of symptoms above) exclusions for mood disorders/schizoaffective disorder/ organic damage/ substance induced Sx
Principles of Cognitive Therapy for Anxiety Disorders A cognitive model is required from which to empirically derive effective treatments You are not mad – you are normal Either it is real or you believe it to be real How you appraise events affects how you feel Test it out – drop your safety-seeking behaviours It’s not what you think, it’s how you think
Morrison (1998) Triggers Auditory Hallucinations Mood & Physiology Safety Behaviours Misinterpretation of Hallucinatory Experience
Cultural acceptability? if someone misinterprets their racing thoughts or palpitations as a sign of alien control or persecution via telekinesis, they will be classified as delusional, whereas misinterpretation of the same sensations as a sign of impending madness or a heart attack would be regarded as indicative of panic disorder a benign lump in one's skin may be misinterpreted as a sign of cancer by a hypochondriacal patient, but the misinterpretation of the same stimuli as being a transmitter or homing device installed by the secret police would be more likely to result in a patient being regarded as psychotic
Experiences that worry me Hear whispering and laughing See bodies See people staring What I make of it They might be ghosts I must be going mad They might harm me What I make of the self / world I should be in total control I am bad Need to be alert for danger Other people cannot be trusted How I feel scared agitated angry sad What I do Try to stay in control of thoughts Hide from ghosts Look out for things happening to me Early experiences Baby brother died, mum blamed me Sexually abused aged 14 Dad horrible to me
Video EFTB formulation for voices
What is changed during CT for people with psychosis / PEs? Appraisals of, and responses to, psychotic experiences Whatever is put on the problem list! Conviction in, frequency of, preoccupation with and distress in response to PEs Can change occurrence of PEs. However, the aim is to change relationship to PEs, making them less significant / distressing e.g. voices may be reattributed as intrusive memories or thoughts (and disappear), but this is a side-effect of developing a less distressing explanation
What is changed during CT for people with psychosis / PEs? Implication of model is that trying to eliminate PEs in people with a diagnosis of schizophrenia would be like trying to eliminate body sensations in patients with panic disorder or intrusive thoughts in patients with OCD Also, normal experiences with understandable consequences due to misinterpretation RATHER THAN AN ILLNESS
I don’t think it’s [CBT] used to eliminate them altogether its knowing why you get the voices erm…how to deal with them basically” (7)
Intervention - Process develop therapeutic relationship assessment establish shared problem list translate into ‘smart’ goals formulation interventions derived from formulation relapse prevention
Intervention Formulation driven Based on cognitive model Follow principles of CT Follow session structure of CT
Intervention – default assumptions Can develop a therapeutic relationship relatively quickly The assessment process, establishing shared problem list, translating into ‘smart’ goals and developing formulation are inherently engaging for most people – collaboration and cards on table We can develop these quickly (e.g. by session 2-6) Formulation is useful for: demonstrating/promoting understanding, validating experiences and selecting change strategies, but it is not an intervention strategy on it’s own Change strategies such as behavioural experiments and verbal reattribution methods are what produce changes Structure and homework are necessary for making process explicit and facilitating learning
Engagement Interventions should be informed by client feedback Normalising of psychotic symptoms should be used to reduce stigma and improve engagement CBT should require consistent collaboration throughout the sessions The rationale of CBT should be explained and demonstrated to the client
CBT should aim to reduce distress and improve quality of life CBT should aim to elicit hope in recovery Session structure and content should be decided jointly between client and therapist Agreed short and long-term goals should underpin the intervention Guided discovery should be used to help the client gain understanding Goals should be SMART (Specific, Measurable, Achievable, Realistic and Time limited) Over the course of therapy a client should work towards becoming their own therapist Socratic questioning, diaries and monitoring procedures should help the client reflect upon and explore new meanings about their thinking, behaviour and context Structure and principles
Formulation A good collaborative relationship must be formed to help develop a comprehensive formulation A formulation should be developed and used to outline a treatment plan A cognitive-behavioural maintenance cycle should be devised and used to set targets for intervention
Assessment and model CBT should be idiosyncratic to the individual client CBT should examine the role that behaviours have in triggering and maintaining the clients difficulties CBT should help a client to identify and elicit those thoughts, images and beliefs which are fundamental to their distress (i.e. the key cognitions) CBT ought to elicit and examine behavioural patterns such as “safety seeking behaviours” in relation to the relevant emotions associated with them
Homework ‘Homework’ should be a ‘standing’ item on the agenda Homework assignments ought to act as a bridge between therapy and the real world
Change strategies Logging pros and cons should be used to explore voices With CBT the client should be supported to explore alternative explanations of experiences that may be more adaptive and less distressing Beliefs in omniscience and omnipotence of command hallucinations should be explored and debated Experiments should be devised to test beliefs by modifying safety behaviours
Therapist assumptions Therapists should believe that many people experience psychotic-like symptoms without feeling distressed by them Therapists ought to believe that delusions can be quite understandable Therapists should believe that it is not the hallucination or the delusion per se that is clinically relevant but the amount of distress or disability associated with it Therapists ought to view most symptoms of psychosis as quite common in the normal population
Therapists should not assume Therapists should NOT believe that clients with psychosis are very different to clients with other mental health difficulties Therapists should NOT believe that there is a clear boundary between being mentally unwell and mentally healthy
Differences Check if involved in symptoms Make allowances for memory & attention Written copies of hw tasks, rationale etc Session summary sheets Shorter, more frequent sessions Importance of tape as homework Importance of structure & instilling process Shorter agenda Importance of therapeutic relationship & engagement Pacing
Assessment Elicit information to flesh out formulation Standard cognitive behavioural assessment Experiences – interpretations – responses Use blank conceptualisation as guide