Download
1 / 22
230 likes | 702 Vues
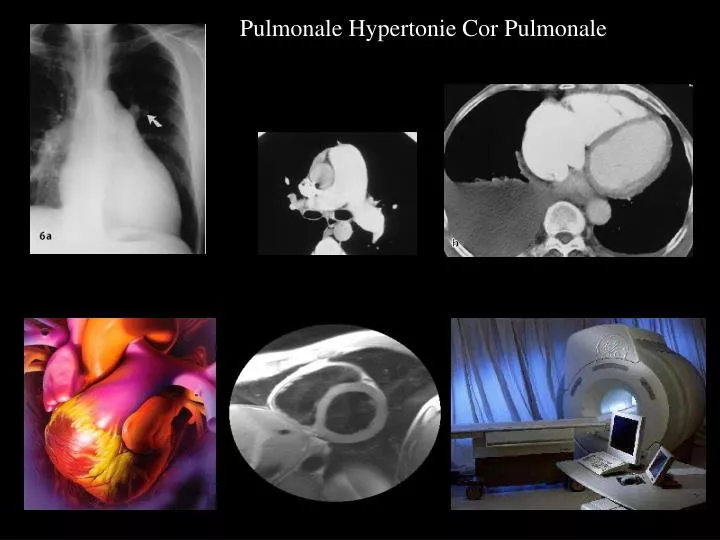
Pulmonale Hypertonie Cor Pulmonale. 1a-b:PPH Cor pulmonale Grad I 2a-e: Grad III. Pulmonalinsuffizienz Dilataton des Konus. DCM mit EF 32 % unklare Belastungsstenokardie. Adenosin- Sressperfusion zur Ischämiediagnostik.

E N D
Adenosin- Sressperfusion zur Ischämiediagnostik Inferiorseptale Ischämie mit initialer verminderter Kontrastaufnahme (dunkles Areal)
TL 201 Myokardszintigraphie links laterodorsaler Perfusionsdefekt Adenosin Stressuntersuchung Ruheredistribution
Stressperfusion mit Adenosin Ischämie der lateralen linksventrikulären Herzwand Kardio-MRT Dynamische Bolusphase Myokardszinthigraphie
1.Stenose der linken A. coronaria circumflexa 2. Erfolgreiche Stenteinlage • S
Late Enhancement zur Infarkt/Narbendiagnostik gesamte Ausdehnung visualisierbar
Unterscheidung Dilatative KHK und DCM Dilatative KHK und DCM zeigen Ventrikelvergrösserung und herabgesetzte EF < 50% Dilatative KHK zeigt fast immer infarkttypisches Late Enhancement DCM : • 59% zeigt kein LE • 28% intramyokardiales LE • 13% infarkttypisches LE Fazit: Bei Patienten ohne infarkttypisches LE kann evtl. auf die Katheteruntersuchung verzichtet werden