Download
1 / 31
310 likes | 368 Vues
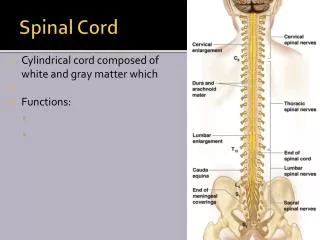
Clinico-Radiological Profile of Spinal Cord Multiple Sclerosis. Glenn H. Roberson Bhavik N. Patel Asim K. Bag. University of Alabama at Birmingham, Birmingham, AL, USA. Glenn H. Roberson: Involved in clinical trials sponsored by Guerbet LLC & Wyeith Pharmaceuticals

E N D
Clinico-Radiological Profile of Spinal Cord Multiple Sclerosis Glenn H. Roberson Bhavik N. Patel Asim K. Bag University of Alabama at Birmingham, Birmingham, AL, USA
Glenn H. Roberson: Involved in clinical trials sponsored by Guerbet LLC & Wyeith Pharmaceuticals Bhavik N. Patel: No disclosure Asim K. Bag: Involved in clinical trials sponsored by ACRIN & Guerbet LLC
Introduction • Multiple sclerosis (MS) has extensive disease burden • MS affects approximately 350,000 individuals in the United States • Typically between the ages of 18 and 45 Medical Clinics of North America 2009;93:451-476
Introduction • Initial MRI diagnosis of MS does not include spinal cord MRI findings • Spinal cord is involved in >90% of MS patients • Asymptomatic cord lesions are found in 30% to 40% of patients • Spinal cord imaging is very important to identify disease progression in time and space Neuroimaging Clinics of North America 2009;19:81-99
Purpose • To identify radiologic pattern of spinal cord involvement in MS • To correlate radiologic findings with clinical symptoms
Materials & Methods: Patients • Retrospective identification of all consecutive patients with abnormal T2 signal in the spinal cord with radiologic concern for MS between 2004 and 2009 • Inclusion criteria • Patients who meet the Revised McDonald MS Diagnostic Criteria were included in this study
Materials & Methods: MRI sequences • Axial • T1 • T2 • STIR • T1+c • Sagittal • T1 • T2 • STIR • T1+c
Materials & Methods: Lesion Characterization • Number of lesions per patient • Involvement pattern of the cord (anterior, posterior, central and diffuse) • Location (cervical, thoracic and lumbar) • Length of lesions • Enhancement pattern
Materials & Methods: Clinical Evaluation • Demography of the patient (age, sex and race) • Clinical presentation • Pattern of disease course
Materials & Methods • Association between lesion location and distribution with symptoms • Association between lesion load and disease course
Results • 544 patients were identified with spinal cord T2 abnormality with radiologic concern for MS • Only 166 patients met the Revised McDonald MS Diagnostic Criteria
Results: Demography • Age range: 17-75 • Male:Female 1:12.9 • More common in Caucasian than African-American (1.84:1)
Results: Clinical presentations • Sensory 42.77% • Motor 37.95 % • Gait 21.68 % • Bladder 12.65 % • No Spinal symptom 12.65 % • Lhermitte 3.01 %
Results: Clinical Course • Relapsing remitting 71.68% • Secondary progressive 24.09% • Primary progressive 0% • Progressive relapsing 0% • Neuromyelitis optica 4.21% Diagram
Results: Lesion loads & disease course • Relapsing-remitting • Average number of lesion 2.20 (range 1 to 7) • Secondary-progressive • Average number of lesion 2.14 (range 1 to 5)
Results: Lesion Characterization 166 patients had total 340 lesions • Location • 46.47% posterior • 27.94% anterior • 22.35% central • 3.23% diffuse • Enhancement • 4.4% • Lesion length • Mean 18.2 mm [range3-108 mm] • Average number of lesions per patient • 2.04
Imaging example Sagittal & Axial T2
Imaging example Sagittal & Axial STIR
Imaging example Sagittal & Axial T2
Imaging example Sagittal & Axial STIR
Imaging example Sagittal & Axial STIR
Imaging example Sagittal T1, T2 & STIR
Imaging example Pre- & post-contrast axial and sagittal T1
Results: Lesion Location • Number of lesions in this bar diagram exceeds 340 as some of the lesions involved more than one segments • Only 7 patients had isolated thoracic spine involvement
Results • No association between lesion location and • Sensory symptoms • Bladder symptoms • Motor symptoms
Results • All patients with posterior column signs, positive Romberg test and gait abnormality had posterior lesions
Source: http://en.wikipedia.org/wiki/File:Spinal_cord_tracts_-_English.svg
Limitations • The study is based on retrospective analysis of data • There is a component of selection bias as the study patients were identified from prior MRI
Conclusion • Demography • Age of presentation 17-75 • Predominantly in women (13:1) • Clinical Presentation • Most common presentation is sensory symptoms • Relapsing-remitting is the most common clinical course
Conclusion • Radiologic appearance • Cervical spinal cord is most commonly involved • Posterior spinal cord is involved most commonly • Mean lesion length is 18.2 mm • Enhancement is rare • Clinico-radiologic correlation • Posterior column signs and gait abnormality are associated with posteriorly located lesions • Average number of lesions is similar in relapsing-remitting and secondary progressive MS