Download
1 / 67
770 likes | 1.57k Vues
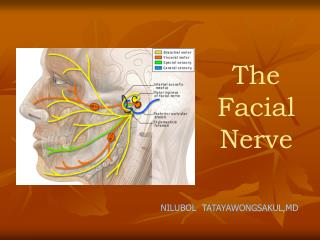
Facial nerve injury. Jihan AL Maddah. Anatomy. Facial nerve is a mixed nerve, having a motor root and a sensory root. Motor root supplies all the mimetic muscles of the face which develop from the 2 nd brachial arch. Anatomy. Sensory root “ nerve of Wrisberg ” carries:

E N D
Facial nerve injury Jihan AL Maddah
Anatomy • Facial nerve is a mixed nerve, having a motor root and a sensory root. • Motor root supplies all the mimetic muscles of the face which develop from the 2nd brachial arch.
Anatomy Sensory root “nerve of Wrisberg” carries: • taste fibers from the anterior 2/3 of the tongue • Secretomotor fibers to the lacrimal, submandibular and sublingual glands as well as those in the nose and palate. • General sensation from the concha and retro-auricular skin.
Anatomy: Nucleus • Pons (motor). • Pre-central gyrus. Upper part of the nucleus: • Upper face • Involuntary emotional movements • Thalamus
Anatomy: Course • Motor fibers originate VII nucleus • Hooks around VI nucleus • Joined by sensory root (nerve of Wrisberg) • Facial n. leaves the brainstem at ponto-medullary junction • Travels through post. Canal fossa • Enters the IAM. • Traverse the temporal bone through facial canal • Leaves the temporal bone through stylomastoid foramen. • Finally divides into terminal branches.
Anatomy: Branches • Greater superficial petrosal nerve: • Nerve to stapedius: • Chorda tympani: • Comunicating branch: • Posterior auricular nerve: • Muscular branches: • Peripheral branches: “Pes anserinus”
Anatomy: Parts • Intracranial part Pons to IAM • Intratemporal part IAM to stylomastoid foramen • Extracranial part Stylomastoid foramen to peripheral branches
Tensor tympani m. Eustachian tube Epitympanic recess mastoid air cells Facial nerve
Anatomy: Intratemporal segments • Meatal • Labyrinthine • Tympanic, horizontal • Mastoid, vertical
Anatomy: Structure of the nerve • From inside outward: • Axon • Myelin sheath • Neurolimma • Endoneurium • Perineurium • Epineurium
Anatomy: Severity of injury • Saunderland classification: • 1°: Partial block: Neuropraxia • 2°: Loss of axons: axonotemesis • 3°: Injury to the endoneurium: neurotemesis • 4°: Injury to the perineurium: partial transection • 5°: Injury to the epineurium: complete transection • 1 to 3 viral inflammatory disorders • 4-5 surgical, accidental trauma, neoplasms.
History: • Onset: Sudden vs. Gradual • Duration: • Rate of progression: • Recuurent or familial • Associated symptoms • Medical history • Previous surgeries
Physical exam: • Complete vs. incomplete • Segmental vs. uniform involvement • Unilateral vs. bilateral • Cranial nerves assessment • Neurologic evaluation • Cerebellar signs
Physical exam: • Microscopic otoscopy • Complete head and neck exam ( including cranial n., parotid…). • Localization of facial nerve lesion: • Central vs. Peripheral.
Physical exam: • Localization of facial nerve lesion: Peripheral: • Level of nucleus • CPA level: • Bony canal level: Topodiagnostics • Outside the Temporal bone
Physical exam: • Topodiagnostics: to localize VII n lesions • Schirmer’s test: lesion proximal to the geniculate. • Stapedial reflex: lesion above n. to stapidus • Taste test: lesion above chorda tympani n. • Submandibular salivery flow test: Warton’s ducts lesion above the chorda tympani
Causes: • Central: • Brain abscess • Pontine glioma • Poliomyelitis • Multiple sclerosis
Causes: • Intacranial part: • Acoustic neuroma • Meningioma • Metastatic CA • Meningitis
Causes: Intratemporal part: 1) Idiopathic: • Bell’s palsy • Melkersson’s syndrome ( facial paralysis, lip swelling and fissured tongue) 2) Infections: • ASOM • CSOM • Herpes Zoster Oticus
Causes: Intratemporal part: cont. 3) Trauma: • Surgical: Mastoidectomy, Stapedectomy • Accidental:# temporal bone 4) Neoplasms: • Glomusjugularetumour • Facial nerve neuroma • Metastatic CA
Causes: • Extracranial part: • Parotid gland CA • Parotid gland surgery • Parotid gland injury • Neonatal facial nerve injury
Causes: • Systemic: • DM • Hypothyroidism • Uremia • Wegener’s granulomatosis • Sarcoidosis • Leprosy • Leukemia
Labs: • Pure-tune audiometry • Electrophysiologic tests • Imaging tests • Others
Labs: • Electrophysiologic tests: • Nerve Excitability Test: NET • Maximum stimulation Test: MST • Electroneurography: ENoG • Electromyography: EMG
Labs: • Nerve Excitability Test: NET : • Indication: complete paralysis<3wks • Interpretation: < or = 3.5 mA threshold: Prognosis Good • Limitation: Not useful in the 1st 3 days or during recovery.
Labs: • Maximum stimulation Test: MST: • Indication: complete paralysis<3wks • Interpretation: Marked weakness or no muscle contraction: advanced degeneration with guarded prognosis • Limitation: Not Objective.
Labs: • Electroneurography: ENoG : • Indication: complete paralysis<3wks • Interpretation: < 90% degeneration: prognosis is good; > or = 90%: prognosis is question • Limitation: False-positive.
Labs: • Electromyography: EMG • Indication: Acute paralysis less than 1 week or chronic paralysis longer than 2 weeks • Interpretation: • Active mu: intact motor axons • Mu + fibrillation potentials: partial degeneration • Polyphasic mu: regenerating nerve • Limitation: cannot assess degree of degeneration or prognosis for recovery.
Complications: • Incomplete recovery • Exposure keratitis • Synkinesis • Tics and spasms • Contractures • Crocodile tears • Frey’s syndrome “gustatory sweating” • Psychological and social problems
Background: • one of the most common neurologic disorders affecting the cranial nerves. • abrupt, unilateral, peripheral facial paresis or paralysis without a detectable cause.
Background: • first described more than a century ago by Sir Charles Bell, • yet much controversy still surrounds its etiology and management. • Bell palsy is certainly the most common cause of facial paralysis worldwide.
Incidence: • The incidence of Bell palsy in the United States is approximately 23 cases per 100,000 persons. • Internationally:The incidence is the same as in the United States.
Demographics: • Race: slightly higher in persons of Japanese descent. • Sex: No difference exists • Age: highest in persons aged 15-45 years. Bell palsy is less common in those younger than 15 years and in those older than 60 years.
Pathophysiology: • Main cause of Bell's palsy is latent herpes viruses (herpes simplex virus type 1 and herpes zoster virus), which are reactivated from cranial nerve ganglia. • Polymerase chain reaction techniques have isolated herpes virus DNA from the facial nerve during acute palsy.
Pathophysiology: • Inflammation of the nerve initially results in a reversible neurapraxia, • Herpes zoster virus shows more aggressive biological behaviour than herpes simplex virus type 1 • Other causes: vascular ischemia, hereditary, autoimmune disorder
History: • The most alarming symptom of Bell's palsy is paresis • Up to three quarters of affected patients think they have had a stroke or have an intracranial tumour.
History: • The palsy is often sudden in onset and evolves rapidly, with maximal facial weakness developing within two days. • Associated symptoms may be hyperacusis, decreased production of tears, and altered taste.
History: • Patients may also mention otalgia or aural fullness and facial or retroauricular pain, which is typically mild and may precede the palsy. • A slow onset progressive palsy with other cranial nerve deficits or headache raises the possibility of a neoplasm