Download
1 / 1
10 likes | 137 Vues
A Reference Range for Thromboelastographic Parameters in Uncomplicated Pregnancy. Helena Maybury 1 , Patricia Squire 1 , Elysee Hille 2 , Frank Pierik 2 , David Taylor 1 , Sue Pavord 3 , Jason Waugh 1 .

E N D
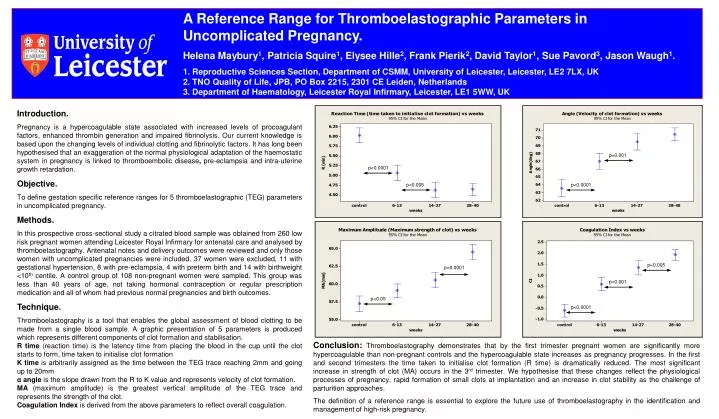
A Reference Range for Thromboelastographic Parameters in Uncomplicated Pregnancy. Helena Maybury1, Patricia Squire1, Elysee Hille2, Frank Pierik2, David Taylor1, Sue Pavord3, Jason Waugh1. 1. Reproductive Sciences Section, Department of CSMM, University of Leicester, Leicester, LE2 7LX, UK 2. TNO Quality of Life, JPB, PO Box 2215, 2301 CE Leiden, Netherlands 3. Department of Haematology, Leicester Royal Infirmary, Leicester, LE1 5WW, UK Introduction. Pregnancy is a hypercoagulable state associated with increased levels of procoagulant factors, enhanced thrombin generation and impaired fibrinolysis. Our current knowledge is based upon the changing levels of individual clotting and fibrinolytic factors. It has long been hypothesised that an exaggeration of the normal physiological adaptation of the haemostatic system in pregnancy is linked to thromboembolic disease, pre-eclampsia and intra-uterine growth retardation. Objective. To define gestation specific reference ranges for 5 thromboelastographic (TEG) parameters in uncomplicated pregnancy. Methods. In this prospective cross-sectional study a citrated blood sample was obtained from 260 low risk pregnant women attending Leicester Royal Infirmary for antenatal care and analysed by thromboelastography. Antenatal notes and delivery outcomes were reviewed and only those women with uncomplicated pregnancies were included. 37 women were excluded, 11 with gestational hypertension, 8 with pre-eclampsia, 4 with preterm birth and 14 with birthweight <10th centile. A control group of 108 non-pregnant women were sampled. This group was less than 40 years of age, not taking hormonal contraception or regular prescription medication and all of whom had previous normal pregnancies and birth outcomes. Technique. Thromboelastography is a tool that enables the global assessment of blood clotting to be made from a single blood sample. A graphic presentation of 5 parameters is produced which represents different components of clot formation and stabilisation. R time (reaction time) is the latency time from placing the blood in the cup until the clot starts to form, time taken to initialise clot formation K time is arbitrarily assigned as the time between the TEG trace reaching 2mm and going up to 20mm α angle is the slope drawn from the R to K value and represents velocity of clot formation. MA (maximum amplitude) is the greatest vertical amplitude of the TEG trace and represents the strength of the clot. Coagulation Index is derived from the above parameters to reflect overall coagulation. p=0.001 p<0.0001 p<0.005 p<0.0001 p=0.005 p<0.0001 p=0.001 p<0.05 p<0.0001 Conclusion: Thromboelastography demonstrates that by the first trimester pregnant women are significantly more hypercoagulable than non-pregnant controls and the hypercoagulable state increases as pregnancy progresses. In the first and second trimesters the time taken to initialise clot formation (R time) is dramatically reduced. The most significant increase in strength of clot (MA) occurs in the 3rd trimester. We hypothesise that these changes reflect the physiological processes of pregnancy, rapid formation of small clots at implantation and an increase in clot stability as the challenge of parturition approaches. The definition of a reference range is essential to explore the future use of thromboelastography in the identification and management of high-risk pregnancy.