Download
1 / 38
1.06k likes | 2.68k Vues
Acute Joint Dislocation. Dr. Abdulrahman Algarni , MD, SSC (Ortho), ABOS Assist. Professor, King Saud University Consultant Orthopedic and Arthroplasty Surgeon. objectives. To know mechanisms of the most common joint dislocations Be able to make the diagnosis

E N D
Acute Joint Dislocation Dr. AbdulrahmanAlgarni, MD, SSC (Ortho), ABOS Assist. Professor, King Saud University Consultant Orthopedic and Arthroplasty Surgeon
objectives • To know mechanisms of the most common joint dislocations • Be able to make the diagnosis • To know and interpret the appropriate x-rays • To know the common complications and how to avoid them
Acute Joint Dislocation • Complete separation of the articularsurface: Joint surfaces are no longer in contact • Position of distal to proximal fragment: Anterior, Posterior, Inferior, Superior
Acute Joint Dislocation • Usually results from high-energy trauma • They occur most frequently in young patients
Clinical Features • Painful; inability to move the limb • Abnormal shape of the joint • The limb is often held in a characteristic position • Careful NV exam before reduction is attempted.
Imaging X-rays • adequate views • Confirm the diagnosis • Rule out fractures i.e. a fracture-dislocation • Reduce before X-rays: knee, ankle • CT scan
Treatment • Urgent reduction: Closed; surgical if failed • Adequate pain relief; muscle relaxant; GA • Imaging after reduction: Post-reduction films • Immobilization • physiotherapy
Complications • Neurovascular injury: Knee, ankle • Avascular necrosis of bone • Recurrent dislocation: shoulder • Heterotopic ossification • Joint stiffness • Secondary osteoarthritis
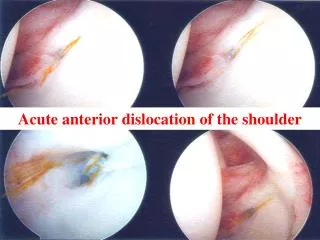
ACUTE SHOULDER DISLOCATION • The most commonly dislocating joint • shallowness of the glenoid socket and wide extraordinary range of motion
ACUTE SHOULDER DISLOCATION • Anterior dislocation is the most common • Posterior dislocation is rare; less than 2%
ANTERIOR SHOULDER DISLOCATION • Fall on the outstretched hand (abduction & external rotation)
ANTERIOR SHOULDER DISLOCATION • The lateral outline of the shoulder may be flattened • Bulge may be felt just below the clavicle
ANTERIOR SHOULDER DISLOCATION • X-rays: antero-posterior and lateral (axillary) views: • Overlapping shadows of the humeral head and glenoidfossa
ANTERIOR SHOULDER DISLOCATION • The head usually lying below and medial to the socket • Rule out greater tubrosity fracture
ANTERIOR SHOULDER DISLOCATION • Avulsion of the antero-inferior glenoid labrum (Bankart lesion). • Indentation of the postero-lateral part of the humeral head (Hill–Sachs lesion)
ANTERIOR SHOULDER DISLOCATION Reduction • Different techniques: Kocher’s, Stimson’s, Milch’s, Hippocratic
ANTERIOR SHOULDER DISLOCATION Reduction • Kocher’s method
ANTERIOR SHOULDER DISLOCATION Complications • Recurrent dislocation: age at first dislocation • Rotator cuff tear: elderly • Axillary nerve injury; neuropraxia • Axillary artery injury • Shoulder stiffness: prolonged immobilization • Unreduced (undiagnosed) dislocation
POSTERIOR SHOULDER DISLOCATION • Indirect force producing marked internal rotation and adduction • Convulsion, or with an electric shock
POSTERIOR SHOULDER DISLOCATION • The diagnosis is frequently missed; more than 50% • The arm is held in internal rotation and is locked in that position • The front of the shoulder looks flat with a prominent coracoid
POSTERIOR SHOULDER DISLOCATION Imaging • The humeral head is medially rotated (electric light bulb) • (The empty glenoid sign) • Axillaryor Scapular view is essential • Rule out fractures; neck, glenoid or lesser tuberosity • CT
HIP DISLOCATION • High energy trauma • posterior (the commonest) • anterior
POSTERIOR HIP DISLOCATION • Road Traffic accident; knee striking against the dashboard • Limb is short, adducted, internally rotated and slightly flexed.
POSTERIOR HIP DISLOCATION • Rule out associated fractures; femur or acetabulum • Rule out sciatic nerve injury
POSTERIOR HIP DISLOCATION • Reduction
POSTERIOR HIP DISLOCATION • Reduction
POSTERIOR HIP DISLOCATION • Reduction; stable • CT scan: the best to demonstrate an acetabular fracture (or any bony fragment)
POSTERIOR HIP DISLOCATION • Sciatic nerve injury; 10% • Avascular necrosis of the femoral head ;10% • If reduction is delayed by more than 12 hours, it rises to over 40% • Hetrotopic ossification
ANTERIOR HIP DISLOCATION • Rare compared with posterior • The leg lies externally rotated, abducted and slightly flexed • Palpable head in the groin
KNEE DISLOCATION • High energy mechanism; RTA • The cruciate ligaments and one or both lateral ligaments are torn
KNEE DISLOCATION • If dislocated joint has reduced spontaneously; swelling and gross instability
KNEE DISLOCATION • If still dislocated; gross deformity
KNEE DISLOCATION • Repeated vascular examination is necessary; popliteal artery injury; risk compartment syndrome • Common peroneal nerve injury: 20 % of cases
KNEE DISLOCATION • X-ray: dislocation, fracture of the tibial spine (cruciate ligament avulsion), avulsion of the fibular styloid (collateral ligament avulsion)
KNEE DISLOCATION • Angiograpy
KNEE DISLOCATION • Urgent reduction • Immediate vascular intervention if needed • Acute or delayed reconstruction of the ligaments
KNEE DISLOCATION Complications • Instability • Stiffness
Summary • Dislocation is an orthopedic emergency and need urgent reduction • Anterior shoulder dislocation is the commonest • Obtain adequate imaging to rule out posterior shoulder dislocation • Acute unstable knee is a knee dislocation until proven otherwise • Always suspect vascular injuries with dislocated knee